

Myocardial recovery in peripartum cardiomyopathy: prospective comparison with recent onset cardiomyopathy in men and nonperipartum women
- PMID: 22196838
- PMCID: PMC3421073
- DOI: 10.1016/j.cardfail.2011.09.009
Myocardial recovery in peripartum cardiomyopathy: prospective comparison with recent onset cardiomyopathy in men and nonperipartum women
Abstract
Background: Whether myocardial recovery occurs more frequently in peripartum cardiomyopathy (PPCM) than in recent onset cardiomyopathies in men and nonperipartum women has not been prospectively evaluated. This was examined through an analysis of outcomes in the Intervention in Myocarditis and Acute Cardiomyopathy 2 (IMAC2) registry.
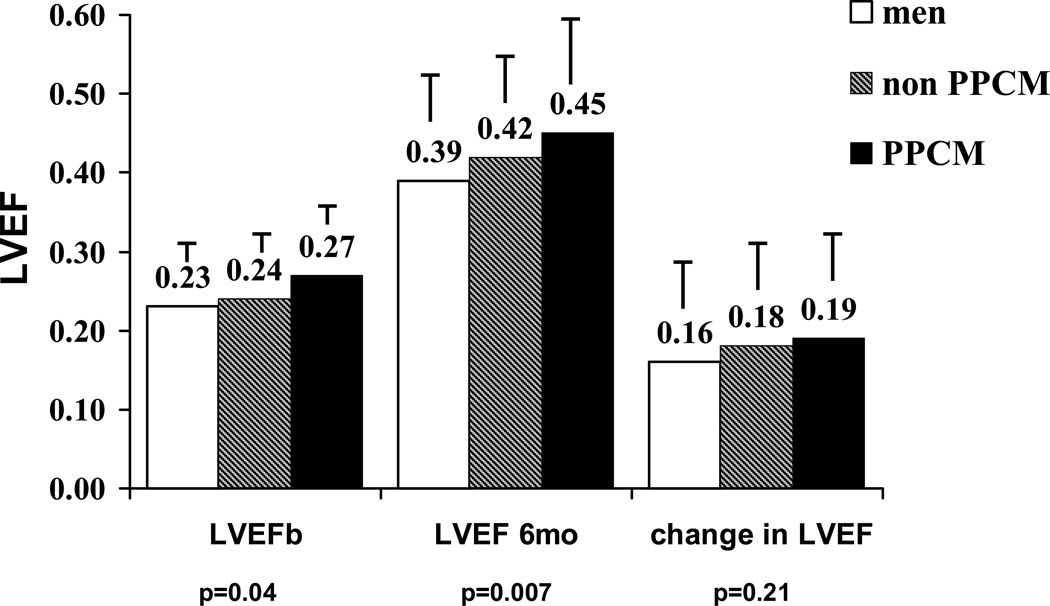
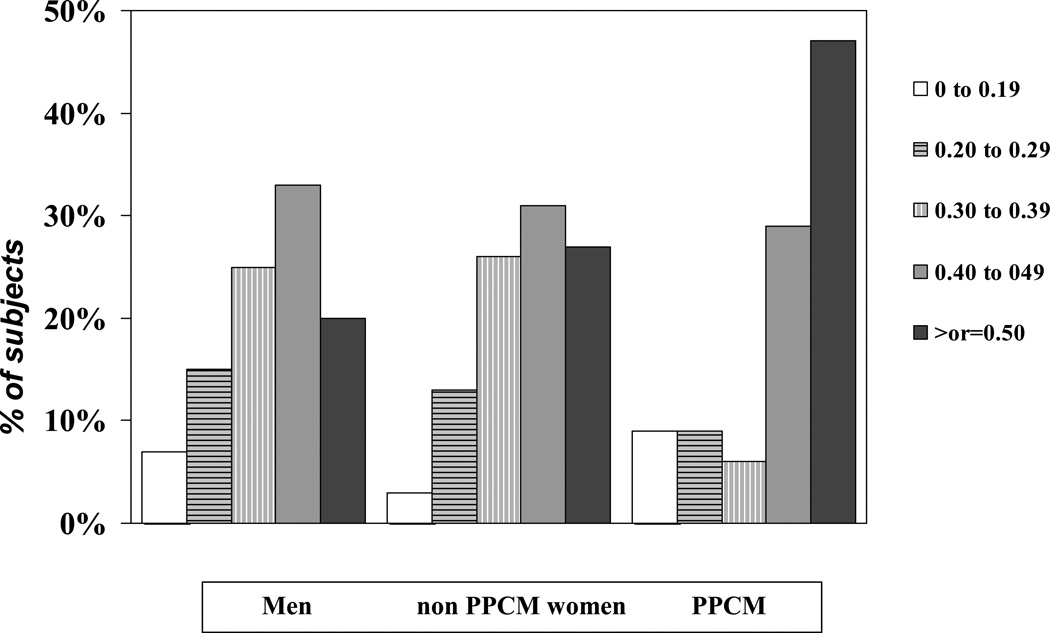
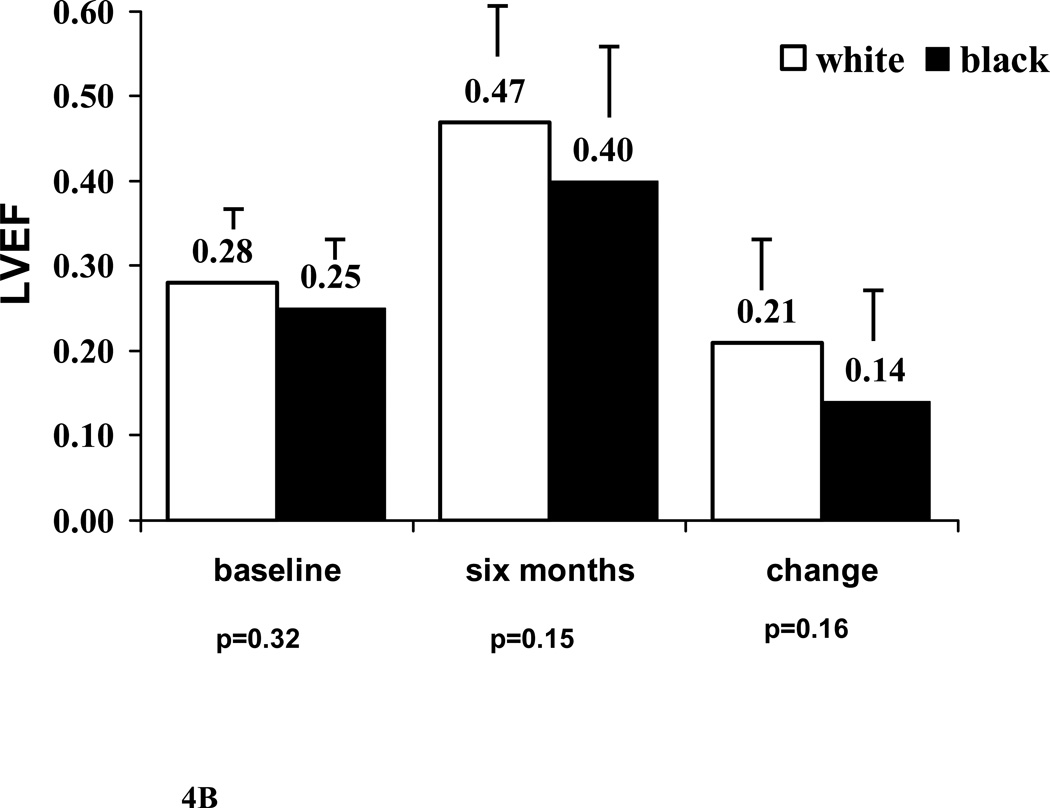
Methods and results: IMAC2 enrolled 373 subjects with recent onset nonischemic dilated cardiomyopathy. Left ventricular ejection fraction (LVEF) was assessed at entry and 6 months, and subjects followed for up to 4 years. Myocardial recovery was compared between men (group 1), nonperipartum women (group 2) and subjects with PPCM (group 3). The cohort included 230 subjects in group 1, 104 in group 2, and 39 in group 3. The mean LVEF at baseline in groups 1, 2, and 3 was 0.23 ± 0.08, 0.24 ± 0.08, and 0.27 ± 0.07 (P = .04), and at 6 months was 0.39 ± 0.12, 0.42 ± 0.11, and 0.45 ± 0.14 (P = .007). Subjects in group 3 had a much greater likelihood of achieving an LVEF >0.50 at 6 months than groups 1 or 2 (19 %, 34%, and 48% respectively, P = .002).
Conclusions: Prospective evaluation confirms myocardial recovery is greatest in women with PPCM, poorest in men, and intermediate in nonperipartum women. On contemporary therapy, nearly half of women with PPCM normalize cardiac function by 6 months.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Pearson GD, Veiled JC, Rahimtoola S, Hsia J, Oakley CM, Hosenpud JD, et al. Peripartum cardiomyopathy: National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) workshop recommendations and review. JAMA. 2000;283:1183–1188. - PubMed
-
- Sliwa K, Hilfiker-Kleiner D, Petrie MC, Buchmann E, Regitz-Zagrosek V, Schaufelberger M, Tavazzi L, et al. Current state of knowledge on etiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. Euro J of Heart Failure. 2010;12:767–778. - PubMed
-
- Mielniczuk LM, Williams K, Davis DR, Tang AS, Lemery R, Green MS, et al. Frequency of Peripartum Cardiomyopathy. Am J Cardiol. 2006;97:1765–1768. - PubMed
-
- Elkayam U, Tummala PP, Rao K, Akhter MW, Karaalp IS, Wani OR, et al. Maternal and fetal outcomes of subsequent pregnancies in women with peripartum cardiomyopathy. New England Journal of Medicine. 2001;344(21):1567–1571. - PubMed
-
- Felker GM, Jaeger CJ, Klodas E, Thiemann DR, Hare JM, Hruban RH, et al. Myocarditis and long-term survival in peripartum cardiomyopathy. Am Heart J. 140:785–789. 200. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
