

Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial
- PMID: 22196944
- PMCID: PMC3273722
- DOI: 10.1016/S0140-6736(11)61335-4
Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial
Abstract
Background: In patients with suspected coronary heart disease, single-photon emission computed tomography (SPECT) is the most widely used test for the assessment of myocardial ischaemia, but its diagnostic accuracy is reported to be variable and it exposes patients to ionising radiation. The aim of this study was to establish the diagnostic accuracy of a multiparametric cardiovascular magnetic resonance (CMR) protocol with x-ray coronary angiography as the reference standard, and to compare CMR with SPECT, in patients with suspected coronary heart disease.
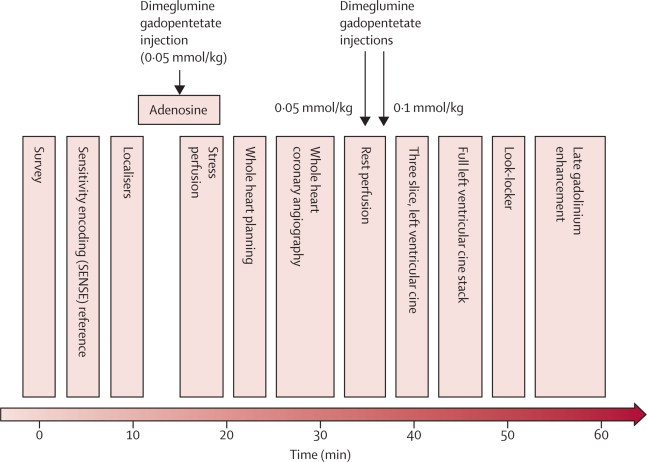
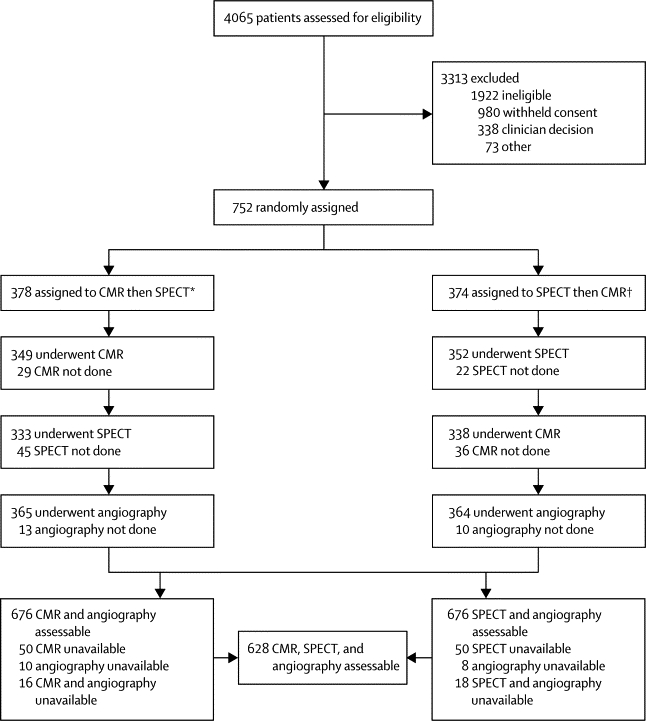
Methods: In this prospective trial patients with suspected angina pectoris and at least one cardiovascular risk factor were scheduled for CMR, SPECT, and invasive x-ray coronary angiography. CMR consisted of rest and adenosine stress perfusion, cine imaging, late gadolinium enhancement, and MR coronary angiography. Gated adenosine stress and rest SPECT used (99m)Tc tetrofosmin. The primary outcome was diagnostic accuracy of CMR. This trial is registered at controlled-trials.com, number ISRCTN77246133.
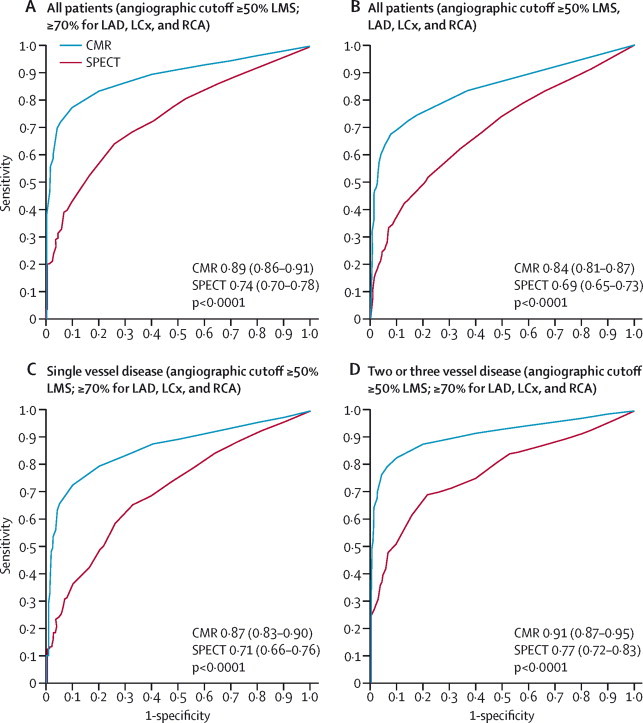
Findings: In the 752 recruited patients, 39% had significant CHD as identified by x-ray angiography. For multiparametric CMR the sensitivity was 86·5% (95% CI 81·8-90·1), specificity 83·4% (79·5-86·7), positive predictive value 77·2%, (72·1-81·6) and negative predictive value 90·5% (87·1-93·0). The sensitivity of SPECT was 66·5% (95% CI 60·4-72·1), specificity 82·6% (78·5-86·1), positive predictive value 71·4% (65·3-76·9), and negative predictive value 79·1% (74·8-82·8). The sensitivity and negative predictive value of CMR and SPECT differed significantly (p<0·0001 for both) but specificity and positive predictive value did not (p=0·916 and p=0·061, respectively).
Interpretation: CE-MARC is the largest, prospective, real world evaluation of CMR and has established CMR's high diagnostic accuracy in coronary heart disease and CMR's superiority over SPECT. It should be adopted more widely than at present for the investigation of coronary heart disease.
Funding: British Heart Foundation.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
What's past is prologue: advances in cardiovascular imaging.Lancet. 2012 Feb 4;379(9814):393-5. doi: 10.1016/S0140-6736(11)61671-1. Epub 2011 Dec 22. Lancet. 2012. PMID: 22196943 No abstract available.
-
CMR versus SPECT for diagnosis of coronary heart disease.Lancet. 2012 Jun 9;379(9832):2145; author reply 2147-8. doi: 10.1016/S0140-6736(12)60936-2. Lancet. 2012. PMID: 22682454 No abstract available.
-
CMR versus SPECT for diagnosis of coronary heart disease.Lancet. 2012 Jun 9;379(9832):2145; author reply 2147-8. doi: 10.1016/S0140-6736(12)60935-0. Lancet. 2012. PMID: 22682455 No abstract available.
-
CMR versus SPECT for diagnosis of coronary heart disease.Lancet. 2012 Jun 9;379(9832):2146; author reply 2147-8. doi: 10.1016/S0140-6736(12)60937-4. Lancet. 2012. PMID: 22682456 No abstract available.
-
CMR versus SPECT for diagnosis of coronary heart disease.Lancet. 2012 Jun 9;379(9832):2146; author reply 2147-8. doi: 10.1016/S0140-6736(12)60938-6. Lancet. 2012. PMID: 22682457 No abstract available.
-
Cardiovascular magnetic resonance for diagnosis of coronary artery disease: quo vadis?Expert Rev Med Devices. 2012 May;9(3):219-24. doi: 10.1586/erd.12.19. Expert Rev Med Devices. 2012. PMID: 22702251
References
-
- WHO Cardiovascular disease. http://www.who.int/cardiovascular_diseases/en/ (accessed March 14, 2011).
-
- NICE Myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction. National Institute for Health and Clinical Excellence. http://www.nice.org.uk/nicemedia/pdf/TA073guidance.pdf (accessed Nov 18).
-
- Mowatt G, Vale L, Brazzelli M. Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction. Health Technol Assess. 2004;8:1–207. - PubMed
-
- Shaw LJ, Bairey Merz CN, Pepine CJ, for the WISE investigators Insights from the NHLBI-sponsored women's ischemia syndrome evaluation (WISE) study: part I: gender differences in traditional and novel risk factors, symptom evaluation, and gender-optimized diagnostic strategies. J Am Coll Cardiol. 2006;47(3 suppl):S4–20. - PubMed
-
- Kim RJ, Wu E, Rafael A. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445–1453. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
