

Changes in global function and regional ventilation and perfusion on SPECT during the course of radiotherapy in patients with non-small-cell lung cancer
- PMID: 22197235
- PMCID: PMC3381888
- DOI: 10.1016/j.ijrobp.2011.07.044
Changes in global function and regional ventilation and perfusion on SPECT during the course of radiotherapy in patients with non-small-cell lung cancer
Abstract
Purpose: This study aimed to (1) examine changes in dyspnea, global pulmonary function test (PFT) results, and functional activity on ventilation (V)/perfusion (Q) single-photon emission computerized tomography (SPECT) scans during the course of radiation (RT), and (2) factors associated with the changes in patients with non-small-cell lung cancer (NSCLC).
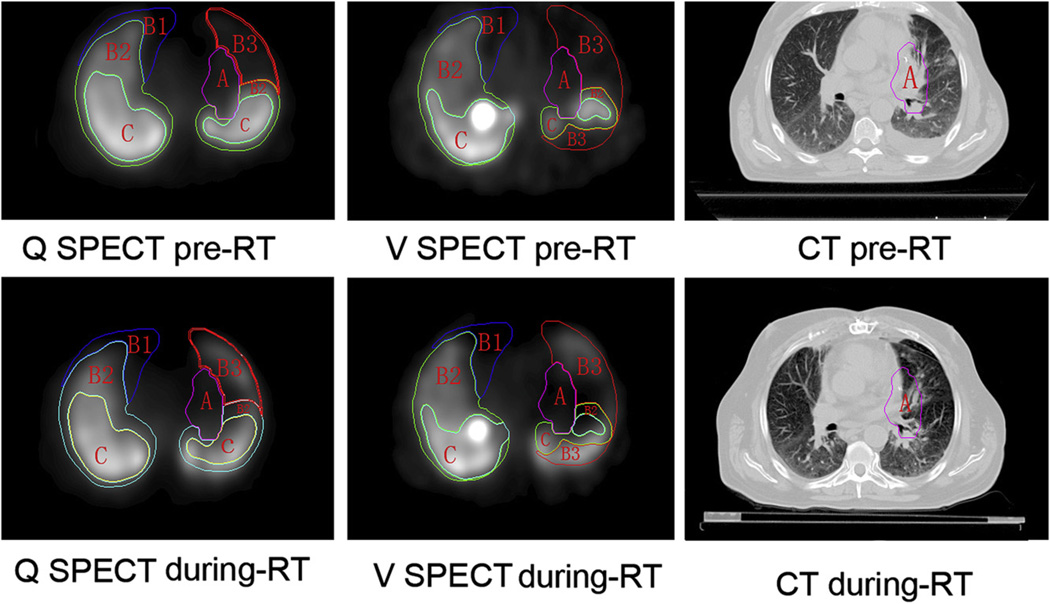
Methods and materials: Fifty-six stage I to III NSCLC patients treated with definitive RT with or without chemotherapy were enrolled prospectively. Dyspnea was graded according to Common Terminology Criteria for Adverse Events version 3.0 prior to and weekly during RT. V/Q SPECT-computed tomography (CT) and PFTs were performed prior to and during RT at approximately 45 Gy. Functions of V and Q activities were assessed using a semiquantitative scoring of SPECT images.
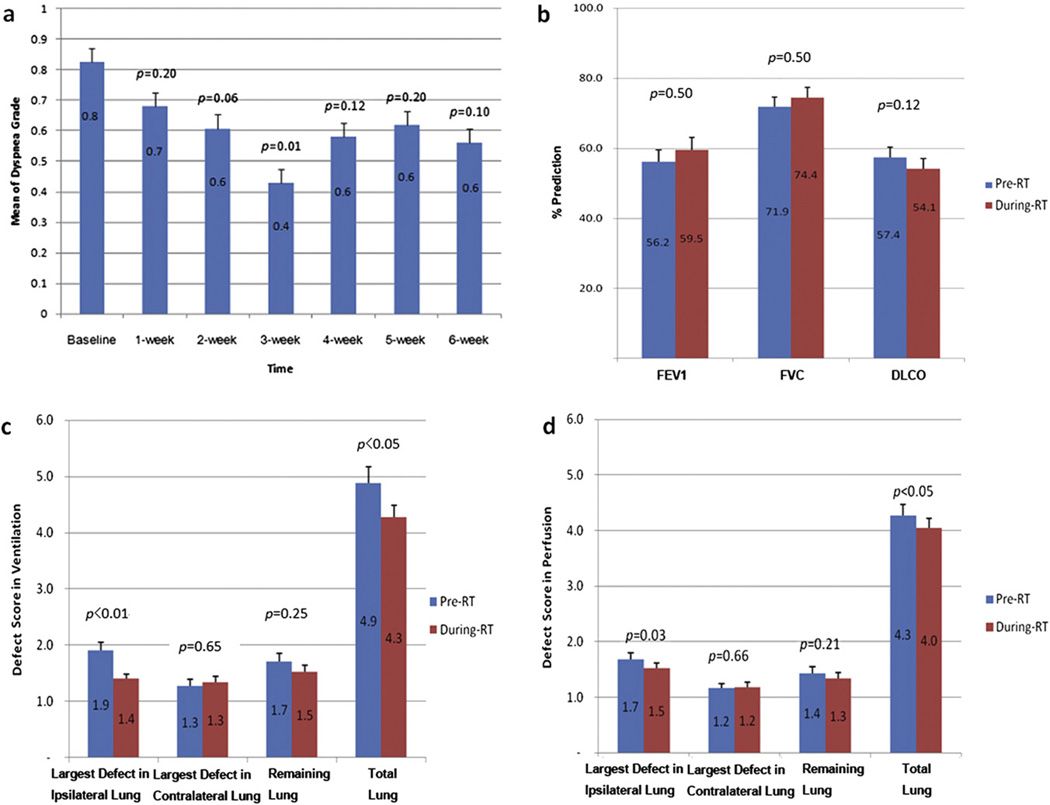
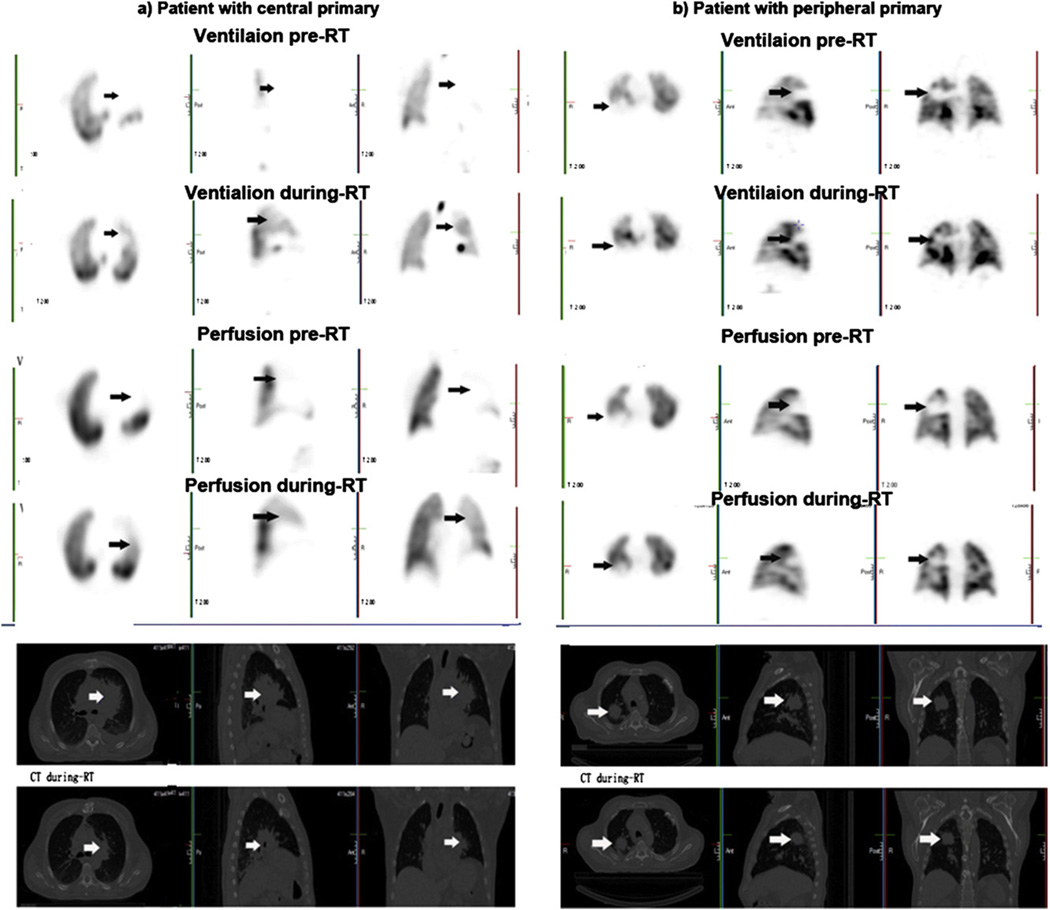
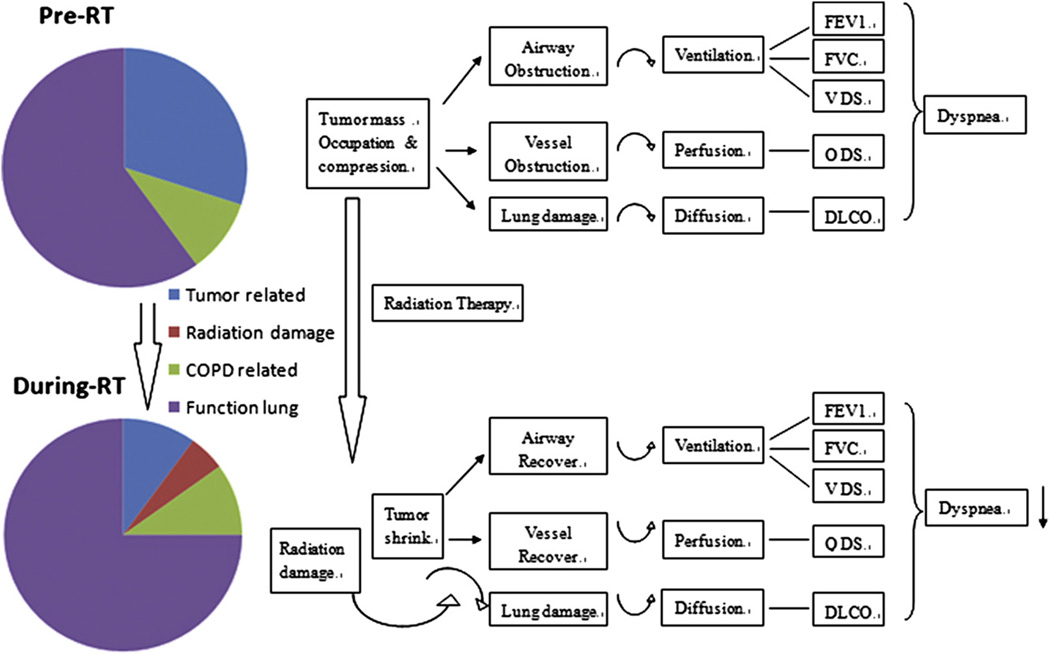
Results: Breathing improved significantly at the third week (mean dyspnea grade, 0.8 vs. 0.6; paired t-test p = 0.011) and worsened during the later course of RT (p > 0.05). Global PFT results did not change significantly, while regional lung function on V/Q SPECT improved significantly after ∼45 Gy. The V defect score (DS) was 4.9 pre-RT versus 4.3 during RT (p = 0.01); Q DS was 4.3 pre-RT versus 4.0 during RT (p < 0.01). Improvements in V and Q functions were seen primarily in the ipsilateral lung (V DS, 1.9 pre-RT versus 1.4 during RT, p < 0.01; Q DS, 1.7 pre-RT versus 1.5 during RT, p < 0.01). Baseline primary tumor volume was significantly correlated with pre-RT V/Q DS (p < 0.01). Patients with central lung tumors had greater interval changes in V and Q than those with more peripheral tumors (p <0.05 for both V and Q DS).
Conclusions: Regional ventilation and perfusion improved during RT at 45 Gy. This suggests that adaptive planning based on V/Q SPECT during RT may allow sparing of functionally recoverable lung tissue.
Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest: none.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Tyldesley S, Boyd C, Schulze K, et al. Estimating the need for radiotherapy for lung cancer: An evidence-based, epidemiologic approach. Int J Radiat Oncol Biol Phys. 2001;49:973–985. - PubMed
-
- Borst GR, De Jaeger K, Belderbos JS, et al. Pulmonary function changes after radiotherapy in non-small-cell lung cancer patients with long-term disease-free survival. Int J Radiat Oncol Biol Phys. 2005;62:639–644. - PubMed
-
- Boersma LJ, Damen EM, de Boer RW, et al. Dose-effect relations for local functional and structural changes of the lung after irradiation for malignant lymphoma. Radiother Oncol. 1994;32:201–209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
