

Medicare part D's impact on antipsychotic drug use and costs among elderly patients without prior drug insurance
- PMID: 22198455
- PMCID: PMC3419531
- DOI: 10.1097/JCP.0b013e31823fb5c4
Medicare part D's impact on antipsychotic drug use and costs among elderly patients without prior drug insurance
Abstract
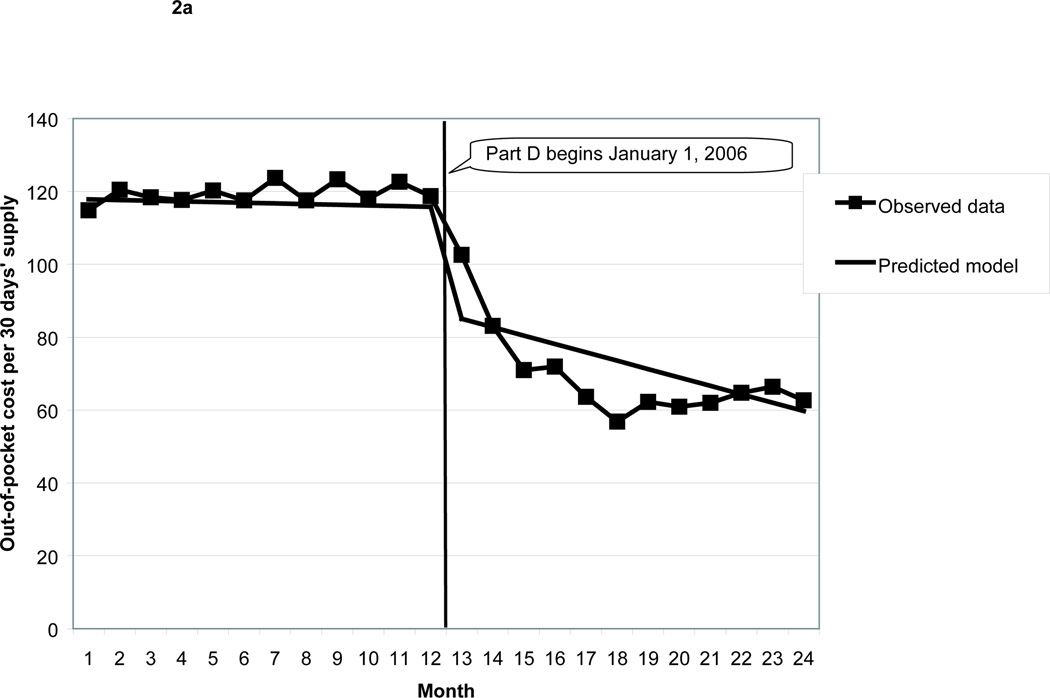
Medicare part D's implementation improved access to and affordability of prescription drugs for the elderly without prior drug insurance. Effects for specific drugs and drug classes are less well understood. We assessed part D's impact on antipsychotic medication (APM) utilization and out-of-pocket costs among elderly without prior drug insurance. Retail pharmacy claims from 3 nationwide pharmacy chains were used to analyze 2 time-series designs: (1) a policy model, to obtain a policymaker's perspective: what was the overall impact of part D on APM use and costs among elderly without drug insurance in 2005 with the opportunity to enroll? And (2) a clinical model, to obtain a clinician's perspective: what would happen to elderly without drug insurance in 2005 who did enroll in part D--would they be able to get APMs? At what cost? Subgroup analyses among part D enrollees evaluated potentially different effects for patients who received a subsidy and patients who used antidementia drugs. In the policy model, part D implementation was associated with a 5% increase in APM use and a 37% reduction in out-of-pocket costs, suggesting a modest need for APMs among all previously uninsured elderly. Patients who did enroll in part D (clinical model) had a 97% increase in APM use and a 62% decrease in out-of-pocket costs, suggesting that patients who needed APMs were able to access them at low cost through the part D program. Part D implementation was associated with increased use and affordability of APMs for the elderly without prior drug insurance.
Conflict of interest statement
Conflicts of interest:
Dr. Polinski is a consultant to Buccaneer Computer Systems and Service, Inc on a contract from the Centers for Medicare and Medicaid Services. Within the past 5 years, Dr. Polinski’s spouse was employed by DePuy Orthopaedics, a subsidiary of Johnson & Johnson, and had Johnson & Johnson stock totaling < $3,100 in value. Dr. Brookhart has received investigator-initiated grant support from Amgen and has participated, without receiving an honorarium, on Amgen advisory boards. He has received consulting fees from Kaiser Permanente and McKesson Health Solutions. Dr. Glynn has a current investigator-initiated unrestricted grant from Astra-Zeneca to study statins, and receives and is co-investigator of a grant from Novartis for the design and monitoring of a randomized trial. Dr. Schneeweiss is a paid member of the Scientific Advisory Board of HealthCore and a consultant to HealthCore, World Health Information Science Consultants, LLC and Research Triangle Institute. Dr. Schneeweiss is Principal Investigator of the Brigham and Women’s Hospital DEcIDE Center on Comparative Effectiveness Research funded by AHRQ and of the Harvard-Brigham Drug Safety and Risk Management Research Center funded by FDA. Within the past 5 years, Dr. Schneeweiss was funded by an investigator-initiated grant from Pfizer which has ended. Opinions expressed here are only those of the authors and not necessarily those of the agencies.
Figures



References
-
- Ketcham JD, Simon KI. Medicare Part D's effects on elderly patients' drug costs and utilization. Am J Manag Care. 2008;14(11 Suppl):SP14–SP22. - PubMed
-
- Lichtenberg FR, Sun SX. The impact of Medicare Part D on prescription drug use by the elderly. Health Aff. 2007;26(6):1735–1744. - PubMed
-
- Yin W, Basu A, Zhang JX, et al. The effect of the Medicare Part D prescription benefit on drug utilization and expenditures. Ann Intern Med. 2008;148(3):169–177. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
