

Central venous pressure and pulmonary capillary wedge pressure: fresh clinical perspectives from a new model of discordant and concordant heart failure
- PMID: 22199422
- PMCID: PMC3233309
Central venous pressure and pulmonary capillary wedge pressure: fresh clinical perspectives from a new model of discordant and concordant heart failure
Abstract
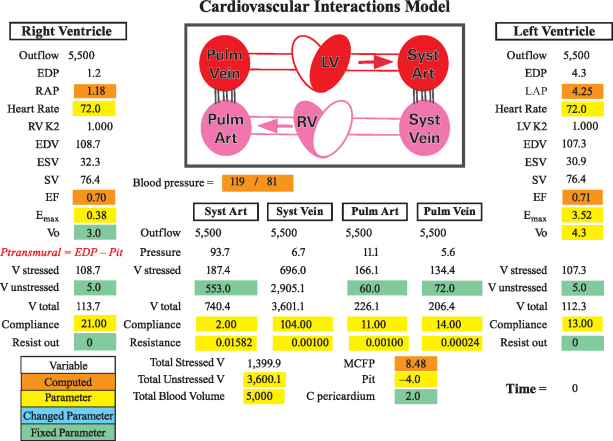
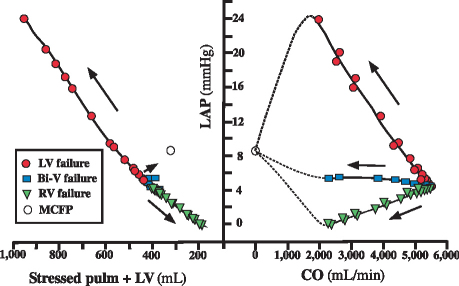
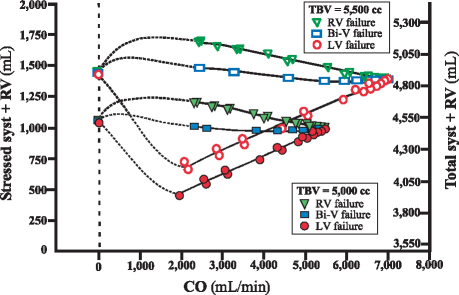
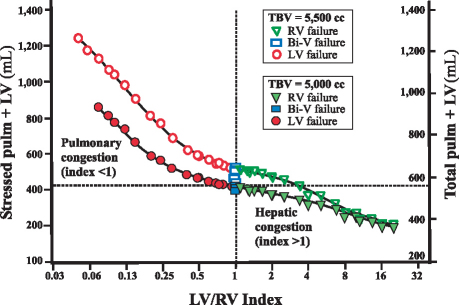
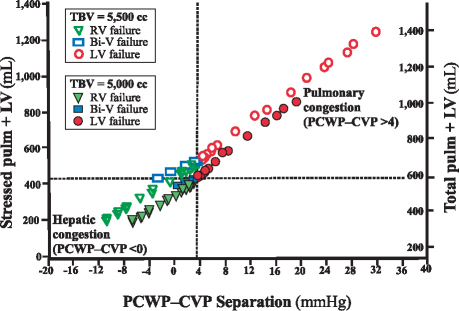
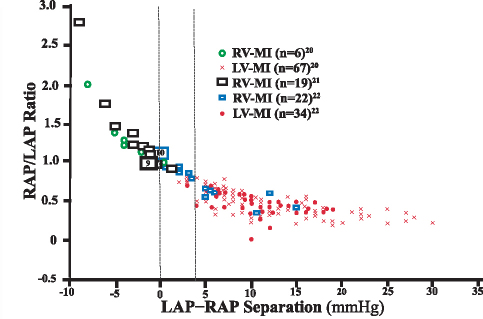
Heart-failure phenotypes include pulmonary and systemic venous congestion. Traditional heart-failure classification systems include the Forrester hemodynamic subsets, which use 2 indices: pulmonary capillary wedge pressure (PCWP) and cardiac index. We hypothesized that changes in PCWP and central venous pressure (CVP), and in the phenotypes of heart failure, might be better evaluated by cardiovascular modeling. Therefore, we developed a lumped-parameter cardiovascular model and analyzed forms of heart failure in which the right and left ventricles failed disproportionately (discordant ventricular failure) versus equally (concordant failure). At least 10 modeling analyses were carried out to the equilibrium state. Acute discordant pump failure was characterized by a "passive" volume movement, with fluid accumulation and pressure elevation in the circuit upstream of the failed pump. In biventricular failure, less volume was mobilized. These findings negate the prevalent teaching that pulmonary congestion in left ventricular failure results primarily from the "backing up" of elevated left ventricular filling pressure. They also reveal a limitation of the Forrester classification: that PCWP and cardiac index are not independent indices of circulation. Herein, we propose a system for classifying heart-failure phenotypes on the basis of discordant or concordant heart failure. A surrogate marker, PCWP-CVP separation, in a simplified situation without complex valvular or pulmonary disease, shows that discordant left and right ventricular failures are characterized by differences of ≥ 4 and ≤ 0 mmHg, respectively. We validated the proposed model and classification system by using published data on patients with acute and chronic heart failure.
Keywords: Blood volume; cardiac output; cardiovascular physiological phenomena; central venous pressure; heart failure/classification/physiopathology; heart ventricles/physiopathology; hemodynamics/physiology; models, cardiovascular; myocardial infarction/physiopathology; pulmonary wedge pressure/physiology; vascular resistance/physiology; ventricular function.
Figures

References
-
- Wood PH. Diseases of the heart and circulation. 2nd ed. Philadelphia: JB Lippincott; 1956. p. 264–317.
-
- Burkhoff D, Tyberg JV. Why does pulmonary venous pressure rise after onset of LV dysfunction: a theoretical analysis. Am J Physiol 1993;265(5 Pt 2):H1819–28. - PubMed
-
- Magder S, Veerassamy S, Bates JH. A further analysis of why pulmonary venous pressure rises after the onset of LV dysfunction. J Appl Physiol 2009;106(1):81–90. - PubMed
-
- Gheorghiade M, Follath F, Ponikowski P, Barsuk JH, Blair JE, Cleland JG, et al. Assessing and grading congestion in acute heart failure: a scientific statement from the acute heart failure committee of the heart failure association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur J Heart Fail 2010;12(5): 423–33. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical