

Post-traumatic cerebral infarction : outcome after decompressive hemicraniectomy for the treatment of traumatic brain injury
- PMID: 22200021
- PMCID: PMC3243842
- DOI: 10.3340/jkns.2011.50.4.370
Post-traumatic cerebral infarction : outcome after decompressive hemicraniectomy for the treatment of traumatic brain injury
Abstract
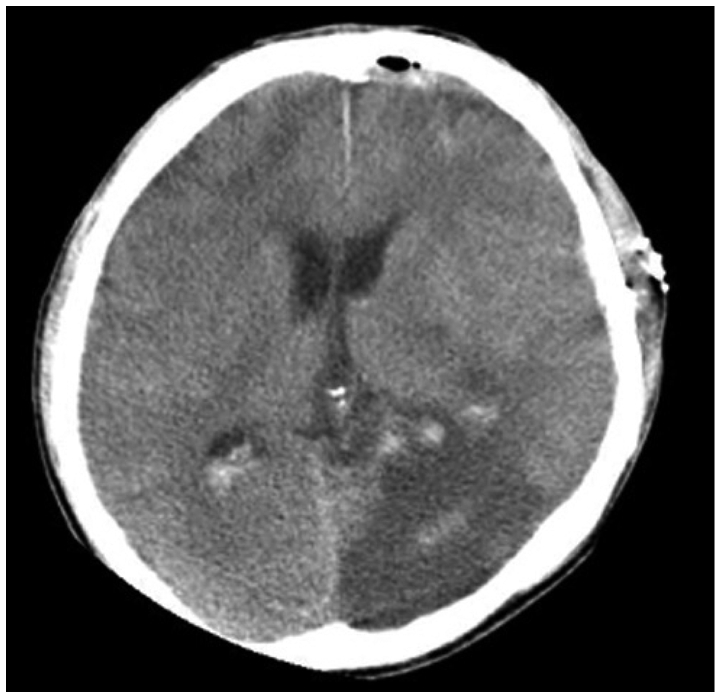
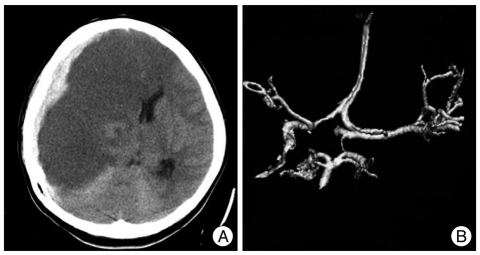
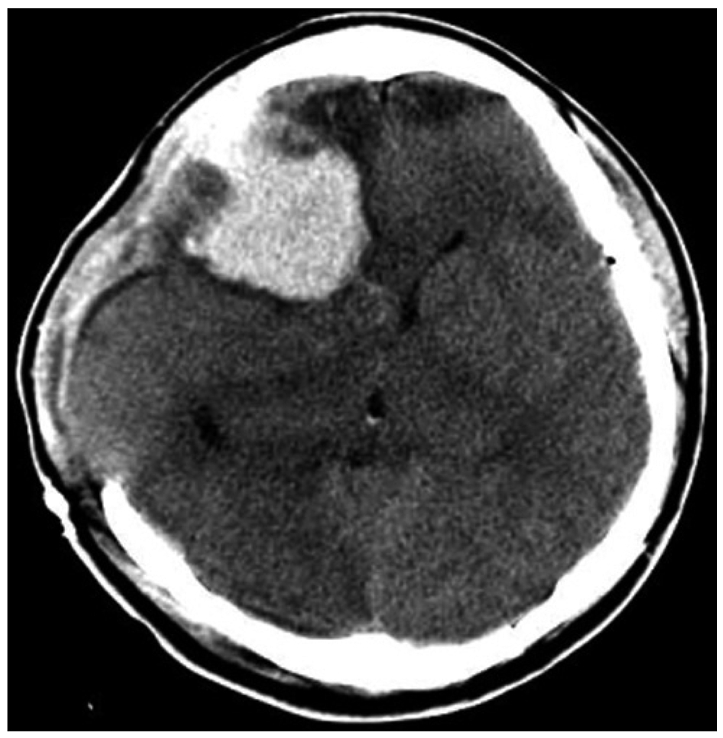
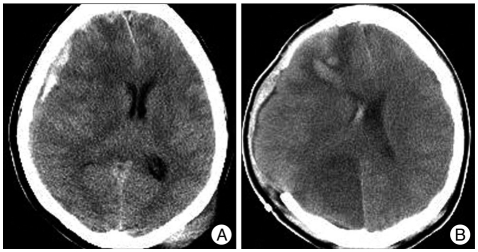
Objective: Posttraumatic cerebral infarction (PTCI), an infarction in well-defined arterial distributions after head trauma, is a known complication in patients with severe head trauma. The primary aims of this study were to evaluate the clinical and radiographic characteristics of PTCI, and to assess the effect on outcome of decompressive hemicraniectomy (DHC) in patients with PTCI.
Methods: We present a retrospective analysis of 20 patients with PTCI who were treated between January 2003 and August 2005. Twelve patients among them showed malignant PTCI, which is defined as PTCI including the territory of Middle Cerebral Artery (MCA). Medical records and radiologic imaging studies of patients were reviewed.
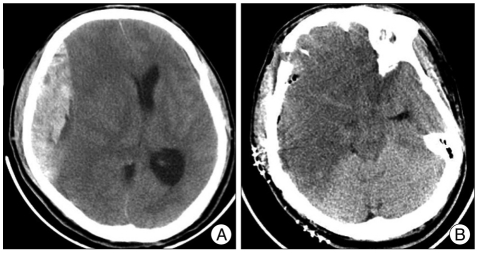
Results: Infarction of posterior cerebral artery distribution was the most common site of PTCI. Fourteen patients underwent DHC an average of 16 hours after trauma. The overall mortality rate was 75%. Glasgow outcome scale (GOS) of survivors showed that one patient was remained in a persistent vegetative state, two patients were severely disabled and only two patients were moderately disabled at the time of discharge. Despite aggressive treatments, all patients with malignant PTCI had died. Malignant PTCI was the indicator of poor clinical outcome. Furthermore, Glasgow coma scale (GCS) at the admission was the most valuable prognostic factor. Significant correlation was observed between a GCS less than 5 on admission and high mortality (p<0.05).
Conclusion: In patients who developed non-malignant PTCI and GCS higher than 5 after head injury, early DHC and duroplasty should be considered, before occurrence of irreversible ischemic brain damage. High mortality rate was observed in patients with malignant PTCI or PTCI with a GCS of 3-5 at the admission. A large prospective randomized controlled study will be required to justify for aggressive treatments including DHC and medical treatment in these patients.
Keywords: Brain trauma; Cerebral infarction; Decompressive craniectomy.
Figures
Similar articles
-
Posttraumatic cerebral infarction after decompressive craniectomy for traumatic brain injury: incidence, risk factors and outcome.Turk Neurosurg. 2017 Jul 23. doi: 10.5137/1019-5149.JTN.20761-17.1. Online ahead of print. Turk Neurosurg. 2017. PMID: 28944947
-
Risk factors for posttraumatic cerebral infarction in patients with moderate or severe head trauma.Neurosurg Rev. 2008 Oct;31(4):431-6; discussion 436-7. doi: 10.1007/s10143-008-0153-5. Epub 2008 Aug 14. Neurosurg Rev. 2008. PMID: 18704527
-
Nationwide survey of decompressive hemicraniectomy for malignant middle cerebral artery infarction in Japan.World Neurosurg. 2014 Dec;82(6):1158-63. doi: 10.1016/j.wneu.2014.07.015. Epub 2014 Jul 18. World Neurosurg. 2014. PMID: 25045787
-
Malignant MCA Infarction: Pathophysiology and Imaging for Early Diagnosis and Management Decisions.Cerebrovasc Dis. 2016;41(1-2):1-7. doi: 10.1159/000441627. Epub 2015 Nov 19. Cerebrovasc Dis. 2016. PMID: 26581023 Review.
-
Hemicraniectomy for malignant middle cerebral artery territory infarction: an updated review.J Neurosurg Sci. 2015 Mar;59(1):73-8. Epub 2014 Nov 25. J Neurosurg Sci. 2015. PMID: 25423133 Review.
Cited by
-
Management of subdural effusion and hydrocephalus following decompressive craniectomy for posttraumatic cerebral infarction in a patient with traumatic brain injury: a case report.BMC Surg. 2019 Feb 27;19(1):26. doi: 10.1186/s12893-019-0489-5. BMC Surg. 2019. PMID: 30813919 Free PMC article.
-
Efficacy and safety of durotomy after decompressive hemicraniectomy in traumatic brain injury.Neurosurg Rev. 2017 Oct;40(4):655-661. doi: 10.1007/s10143-017-0823-2. Epub 2017 Feb 9. Neurosurg Rev. 2017. PMID: 28185018
-
Post-traumatic cerebral infarction following low-energy penetrating craniocerebral injury caused by a nail.J Korean Neurosurg Soc. 2014 May;55(5):293-5. doi: 10.3340/jkns.2014.55.5.293. Epub 2014 May 31. J Korean Neurosurg Soc. 2014. PMID: 25132939 Free PMC article.
-
The Effect of Controlled Decompression for Severe Traumatic Brain Injury: A Randomized, Controlled Trial.Front Neurol. 2020 Feb 18;11:107. doi: 10.3389/fneur.2020.00107. eCollection 2020. Front Neurol. 2020. PMID: 32132972 Free PMC article.
-
Treatment of acute disseminated encephalomyelitis.Curr Treat Options Neurol. 2012 Jun;14(3):264-75. doi: 10.1007/s11940-012-0170-0. Curr Treat Options Neurol. 2012. PMID: 22476745
References
-
- Doerfler A, Engelhorn T, Forsting M. Decompressive craniectomy for early therapy and secondary prevention of cerebral infarction. Stroke. 2001;32:813–815. - PubMed
-
- Eberle BM, Schnüriger B, Inaba K, Gruen JP, Demetriades D, Belzberg H. Decompressive craniectomy : surgical control of traumatic intracranial hypertension may improve outcome. Injury. 2010;41:894–898. - PubMed
-
- Figaji AA, Fieggen AG, Peter JC. Early decompressive craniotomy in children with severe traumatic brain injury. Childs Nerv Syst. 2003;19:666–673. - PubMed
-
- Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R. 'Malignant' middle cerebral artery territory infarction: clinical course and prognostic signs. Arch Neurol. 1996;53:309–315. - PubMed
-
- Harscher S, Reichart R, Terborg C, Hagemann G, Kalff R, Witte OW. Outcome after decompressive craniectomy in patients with severe ischemic stroke. Acta Neurochir (Wien) 2006;148:31–37. discussion 37. - PubMed
LinkOut - more resources
Full Text Sources
