Amylase, lipase, and volume of drainage fluid in gastrectomy for the early detection of complications caused by pancreatic leakage
- PMID: 22200041
- PMCID: PMC3243857
- DOI: 10.4174/jkss.2011.81.6.402
Amylase, lipase, and volume of drainage fluid in gastrectomy for the early detection of complications caused by pancreatic leakage
Abstract
Purpose: Pancreatic leakage is a serious complication of gastrectomy due to stomach cancer. Therefore, we analyzed amylase and lipase concentrations in blood and drainage fluid, and evaluated the volume of drainage fluid to discern their usefulness as markers for the early detection of serious pancreatic leakage requiring reoperation after gastrectomy.
Methods: From January 2001 to December 2007, we retrospectively analyzed data from 24,072 patient samples. We divided patients into two groups; 1) complications with pancreatic leakage (CG), and 2) no complications associated with pancreatic leakage (NCG). Values of amylase and lipase in the blood and drainage fluid, volume of the drainage fluid, and relationships among the volumes, amylase values, and lipase values in the drainage fluid were evaluated, respectively in the two groups.
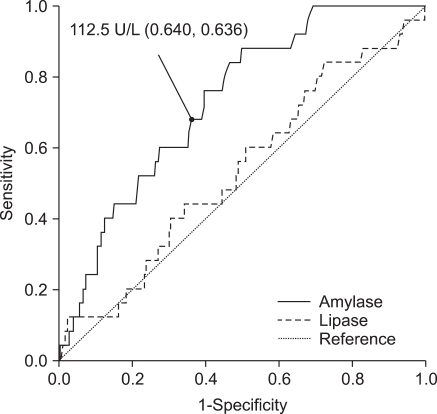
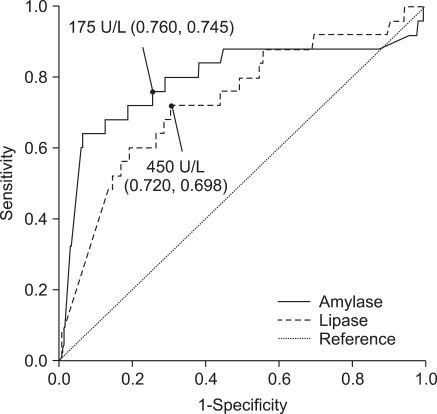
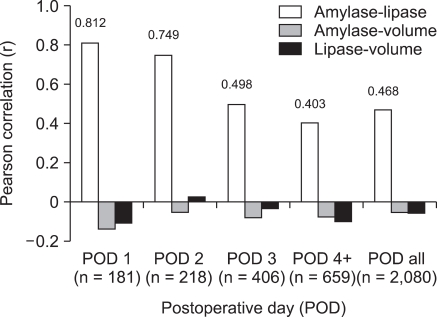
Results: The mean amylase values of CG were significantly higher than those of NCG in blood and drainage fluid (P < 0.05). For lipase, statistically significant differences were observed in drainage fluid (P < 0.05). The mean volume (standard deviation) of the drained fluid through the tube between CG (n = 22) and NCG (n = 236) on postoperative day 1 were 368.41 (266.25) and 299.26 (300.28), respectively. There were no statistically significant differences between the groups (P = 0.298). There was a correlation between the amylase and lipase values in the drainage fluid (r = 0.812, P = 0.000).
Conclusion: Among postoperative amylase and lipase values in blood and drainage fluid, and the volume of drainage fluid, the amylase in drainage fluid was better differentiated between CG and NCG than other markers. The volume of the drainage fluid did not differ significantly between groups.
Keywords: Drainage fluid; Gastrectomy; Pancreatic leakage; Stomach neoplasms.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Sano T, Sasako M, Katai H, Maruyama K. Amylase concentration of drainage fluid after total gastrectomy. Br J Surg. 1997;84:1310–1312. - PubMed
-
- Bonenkamp JJ, Songun I, Hermans J, Sasako M, Welvaart K, Plukker JT, et al. Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. Lancet. 1995;345:745–748. - PubMed
-
- Sasako M, McCulloch P, Kinoshita T, Maruyama K. New method to evaluate the therapeutic value of lymph node dissection for gastric cancer. Br J Surg. 1995;82:346–351. - PubMed
-
- Tanaka K, Miyashiro I, Yano M, Kishi K, Motoori M, Seki Y, et al. Accumulation of excess visceral fat is a risk factor for pancreatic fistula formation after total gastrectomy. Ann Surg Oncol. 2009;16:1520–1525. - PubMed
LinkOut - more resources
Full Text Sources