

Meeting standards of high-quality intensive care unit palliative care: clinical performance and predictors
- PMID: 22202706
- PMCID: PMC3307856
- DOI: 10.1097/CCM.0b013e3182374a50
Meeting standards of high-quality intensive care unit palliative care: clinical performance and predictors
Abstract
Objectives: High-quality care for intensive care unit patients and families includes palliative care. To promote performance improvement, the Agency for Healthcare Research and Quality's National Quality Measures Clearinghouse identified nine evidence-based processes of intensive care unit palliative care (Care and Communication Bundle) that are measured through review of medical record documentation. We conducted this study to examine how frequently the Care and Communication Bundle processes were performed in diverse intensive care units and to understand patient factors that are associated with such performance.
Design: Prospective, multisite, observational study of performance of key intensive care unit palliative care processes.
Settings: A surgical intensive care unit and a medical intensive care unit in two different large academic health centers and a medical-surgical intensive care unit in a medium-sized community hospital.
Patients: Consecutive adult patients with length of intensive care unit stay ≥5 days.
Interventions: None.
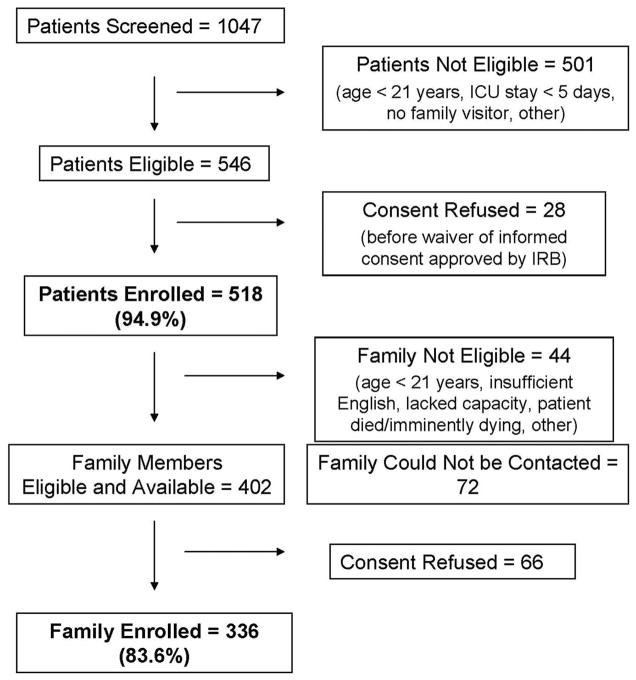
Measurements and main results: Between November 2007 and December 2009, we measured performance by specified day after intensive care unit admission on nine care process measures: Identify medical decision-maker, advance directive and resuscitation preference, distribute family information leaflet, assess and manage pain, offer social work and spiritual support, and conduct interdisciplinary family meeting. Multivariable regression analysis was used to determine predictors of performance of five care processes. We enrolled 518 (94.9%) patients and 336 (83.6%) family members. Performances on pain assessment and management measures were high. In contrast, interdisciplinary family meetings were documented for <20% of patients by intensive care unit day 5. Performance on other measures ranged from 8% to 43%, with substantial variation across and within sites. Chronic comorbidity burden and site were the most consistent predictors of care process performance.
Conclusions: Across three intensive care units in this study, performance of key palliative care processes (other than pain assessment and management) was inconsistent and infrequent. Available resources and strategies should be utilized for performance improvement in this area of high importance to patients, families, and providers.
Conflict of interest statement
Dr. Nelson consulted for the Voluntary Hospital Association, Inc. and Veterans Integrated Service Network 3 of the Department of Veterans Affairs. Dr. Puntillo consulted for Veterans Integrated Service Network 3 of the Department of Veterans Affairs. The remaining authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Measuring intensive care unit palliative care: have we set the bar too low?Crit Care Med. 2012 Apr;40(4):1343-5. doi: 10.1097/CCM.0b013e3182431707. Crit Care Med. 2012. PMID: 22425832 No abstract available.
References
-
- Field MJ, Cassel CK, editors. Approaching Death: Improving Care at the End of Life. Washington, DC: National Academy Press (Institute of Medicine); 1997. - PubMed
-
- Lanken PN, Terry PB, Delisser HM, et al. An official American Thoracic Society clinical policy statement: Palliative care for patients with respiratory diseases and critical illnesses. Am J Respir Crit Care Med. 2008;177:912–927. - PubMed
-
- Truog RD, Campbell ML, Curtis JR, et al. Recommendations for end-of-life care in the intensive care unit: A consensus statement by the American College [corrected] of Critical Care Medicine. Crit Care Med. 2008;36:953–963. - PubMed
-
- Selecky PA, Eliasson CA, Hall RI, et al. Palliative and end-of-life care for patients with cardiopulmonary diseases: American College of Chest Physicians position statement. Chest. 2005;128:3599–3610. - PubMed
-
- [Accessed July 1, 2011];National Priorities Partnership website. Available at: http://www.nationalprioritiespartnership.org/Priorities.aspx.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
