

What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation?
- PMID: 22202708
- PMCID: PMC3307954
- DOI: 10.1097/CCM.0b013e31823bc8bb
What is the role of chest compression depth during out-of-hospital cardiac arrest resuscitation?
Abstract
Background: The 2010 international guidelines for cardiopulmonary resuscitation recently recommended an increase in the minimum compression depth from 38 to 50 mm, although there are limited human data to support this. We sought to study patterns of cardiopulmonary resuscitation compression depth and their associations with patient outcomes in out-of-hospital cardiac arrest cases treated by the 2005 guideline standards.
Design: Prospective cohort.
Setting: Seven U.S. and Canadian urban regions.
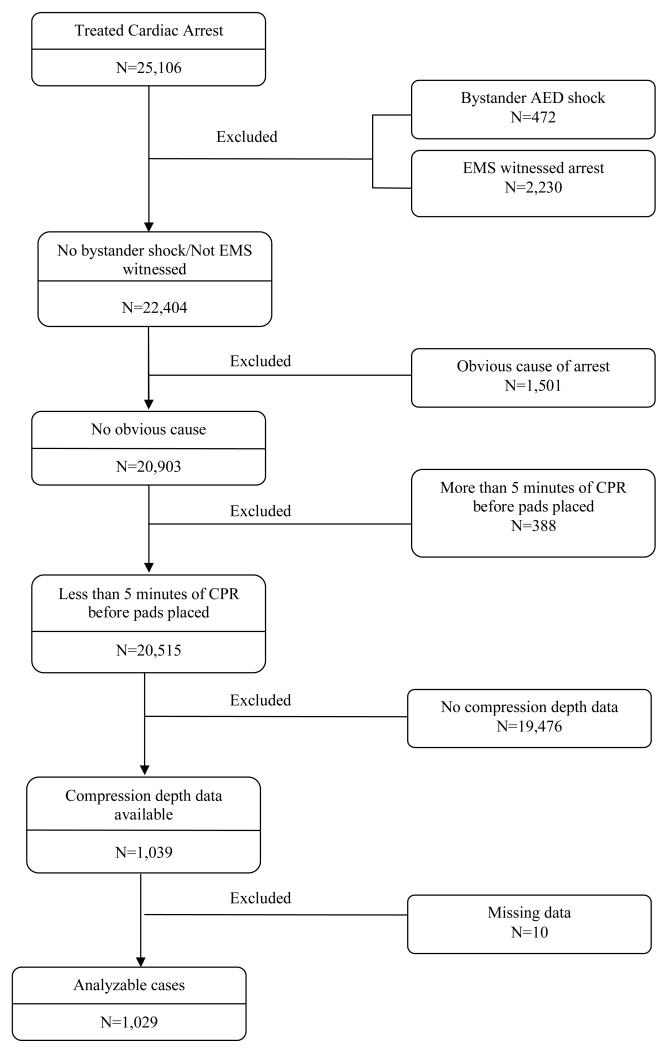
Patients: We studied emergency medical services treated out-of-hospital cardiac arrest patients from the Resuscitation Outcomes Consortium Epistry-Cardiac Arrest for whom electronic cardiopulmonary resuscitation compression depth data were available, from May 2006 to June 2009.
Measurements: We calculated anterior chest wall depression in millimeters and the period of active cardiopulmonary resuscitation (chest compression fraction) for each minute of cardiopulmonary resuscitation. We controlled for covariates including compression rate and calculated adjusted odds ratios for any return of spontaneous circulation, 1-day survival, and hospital discharge.
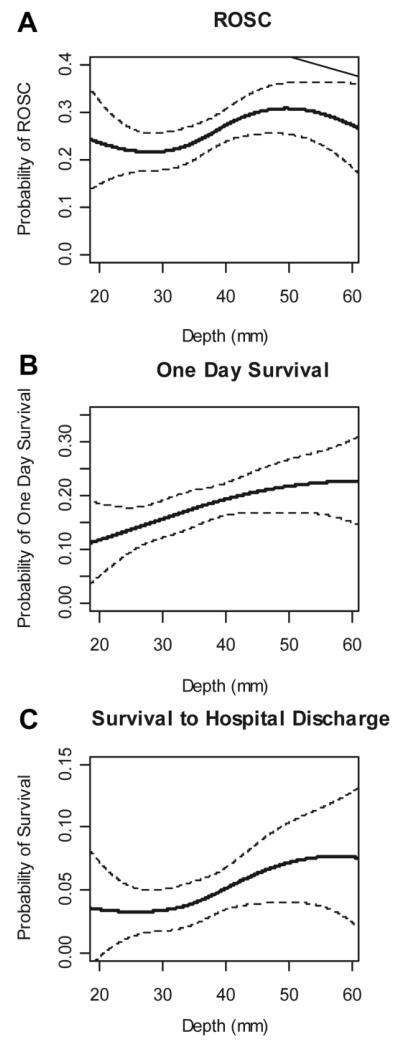
Main results: We included 1029 adult patients from seven U.S. and Canadian cities with the following characteristics: Mean age 68 yrs; male 62%; bystander witnessed 40%; bystander cardiopulmonary resuscitation 37%; initial rhythms: Ventricular fibrillation/ventricular tachycardia 24%, pulseless electrical activity 16%, asystole 48%, other nonshockable 12%; outcomes: Return of spontaneous circulation 26%, 1-day survival 18%, discharge 5%. For all patients, median compression rate was 106 per minute, median compression fraction 0.65, and median compression depth 37.3 mm with 52.8% of cases having depth <38 mm and 91.6% having depth <50 mm. We found an inverse association between depth and compression rate ( p < .001). Adjusted odds ratios for all depth measures (mean values, categories, and range) showed strong trends toward better outcomes with increased depth for all three survival measures.
Conclusions: We found suboptimal compression depth in half of patients by 2005 guideline standards and almost all by 2010 standards as well as an inverse association between compression depth and rate. We found a strong association between survival outcomes and increased compression depth but no clear evidence to support or refute the 2010 recommendations of >50 mm. Although compression depth is an important component of cardiopulmonary resuscitation and should be measured routinely, the most effective depth is currently unknown.
Figures
Comment in
-
Chest compression quality--push hard, push fast, but how deep and how fast?Crit Care Med. 2012 Apr;40(4):1363-4. doi: 10.1097/CCM.0b013e31824102e2. Crit Care Med. 2012. PMID: 22425844 No abstract available.
References
-
- Cummins RO, Ornato JP, Thies WH, Pepe PE. Improving survival from sudden cardiac arrest: the “chain of survival” concept. Circulation. 1991;83:1832–1847. - PubMed
-
- 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112(24 Suppl):IV1–203. - PubMed
-
- Stiell IG, Wells GA, Field BJ, Spaite DW, Nesbitt L, De Maio VJ, et al. Advanced Cardiac Life Support in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2004;351:647–656. - PubMed
-
- Rea TD, Cook AJ, Stiell IG, Powell J, Bigham B, Callaway CW, et al. Predicting survival after out-of-hospital cardiac arrest: role of the Utstein data elements. Ann Emerg Med. 2010;55(3):249–257. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
