

Cardiac risk assessment by gated single-photon emission computed tomography in asymptomatic end-stage renal disease patients at the start of dialysis
- PMID: 22203446
- PMCID: PMC3358562
- DOI: 10.1007/s12350-011-9497-2
Cardiac risk assessment by gated single-photon emission computed tomography in asymptomatic end-stage renal disease patients at the start of dialysis
Abstract
Objectives: This study assessed the impact of cardiac risk assessment using gated single-photon emission computed tomography (SPECT) on cardiac events in end-stage renal disease (ESRD) patients.
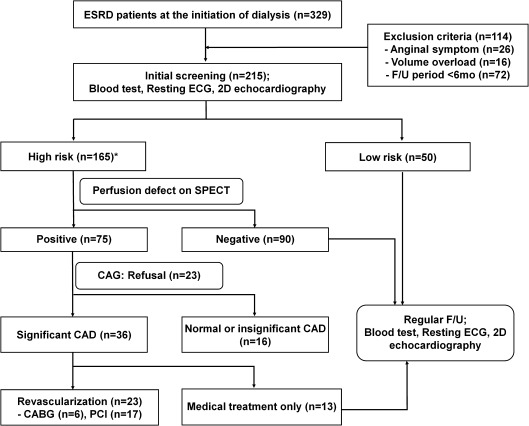
Methods: We evaluated 215 asymptomatic patients who began dialysis between January 2005 and April 2009. Baseline electrocardiography and echocardiography were performed in all the patients. The subjects were stratified into low- and high-risk groups according to the baseline cardiac status, and gated SPECT was additionally recommended for the high-risk patients.
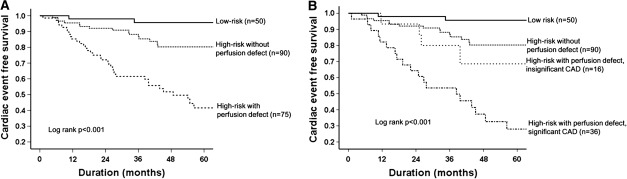
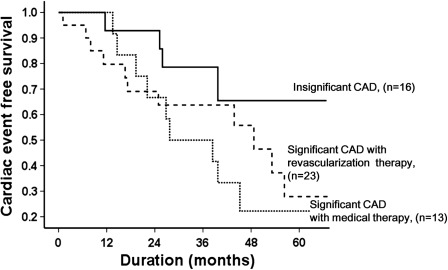
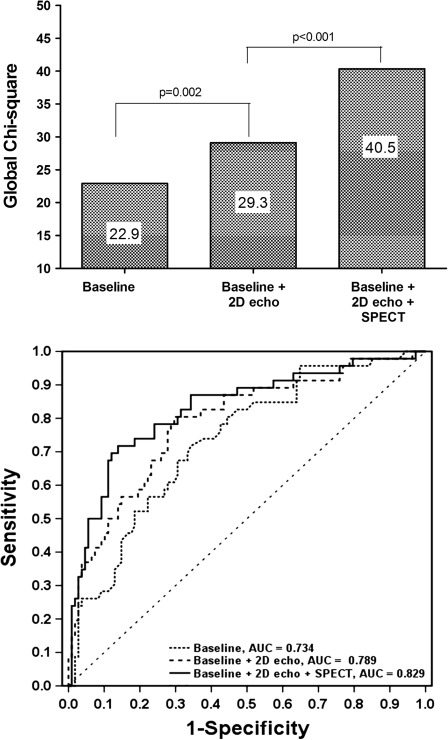
Results: The study population consisted of 50 low- and 165 high-risk patients undergoing SPECT. Among the high-risk patients, 75 (45.5%) showed perfusion defects on SPECT and their overall cardiac-event rate per person-year of follow-up was 15.0%, significantly higher than 4.5% in high-risk group without perfusion defect and 1.2% in low-risk group. The presence of perfusion defect was a significant independent predictor of adverse cardiac events [hazard ratio (HR) 2.11; 95% confidence interval (CI) 1.05-4.24; P = .035]. When gated SPECT was added to the clinical and the echocardiographic variables, the prognostic stratification significantly improved (P < .001). However, coronary revascularization was not associated with improved cardiac event-free survival (HR 0.62; 95% CI 0.26-1.52; P = .296).
Conclusions: Gated SPECT may provide additional prognostic information for cardiac risk stratification, particularly among high-risk patients starting dialysis.
Figures
Comment in
-
Myocardial perfusion SPECT "screening" at the start of dialysis.J Nucl Cardiol. 2012 Jun;19(3):410-1. doi: 10.1007/s12350-012-9524-y. J Nucl Cardiol. 2012. PMID: 22351493 No abstract available.
References
-
- Baig SZ, Coats WC, Aggarwal KB, Alpert MA. Assessing cardiovascular disease in the dialysis patient. Adv Perit Dial. 2009;25:147–154. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
