

Thyroid nodules: risk stratification for malignancy with ultrasound and guided biopsy
- PMID: 22203727
- PMCID: PMC3266587
- DOI: 10.1102/1470-7330.2011.0030
Thyroid nodules: risk stratification for malignancy with ultrasound and guided biopsy
Abstract
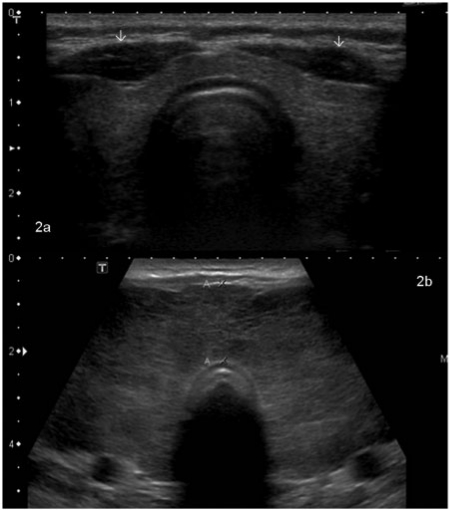
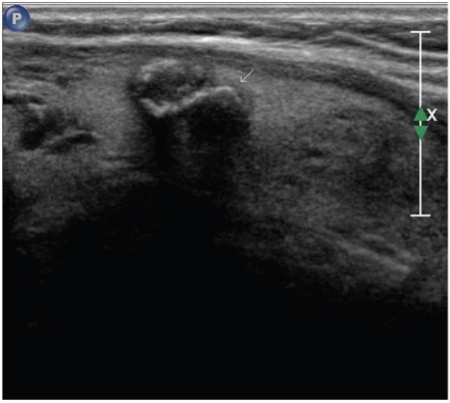
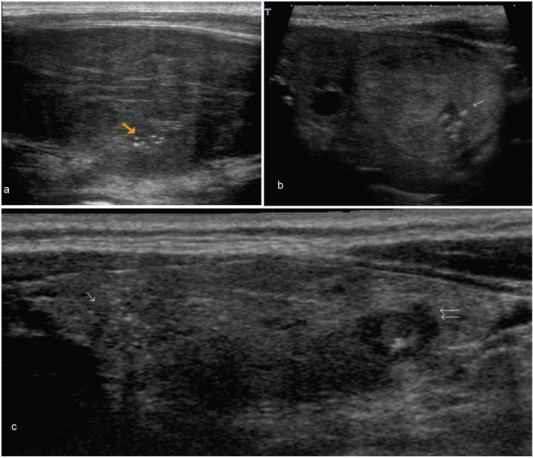
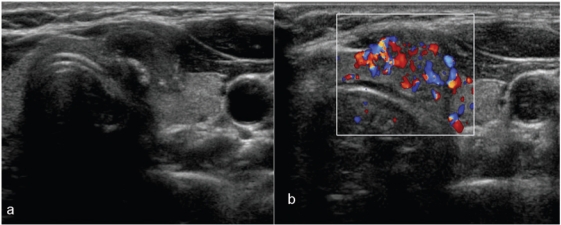
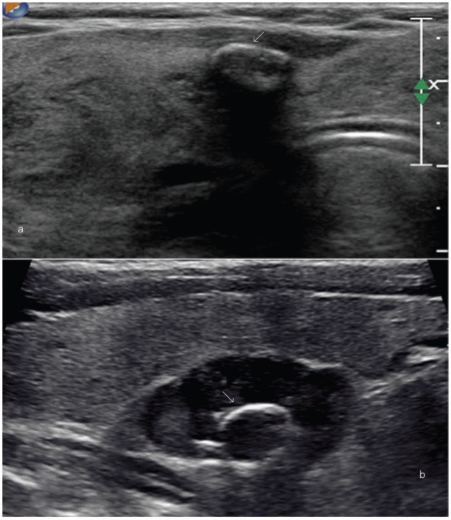
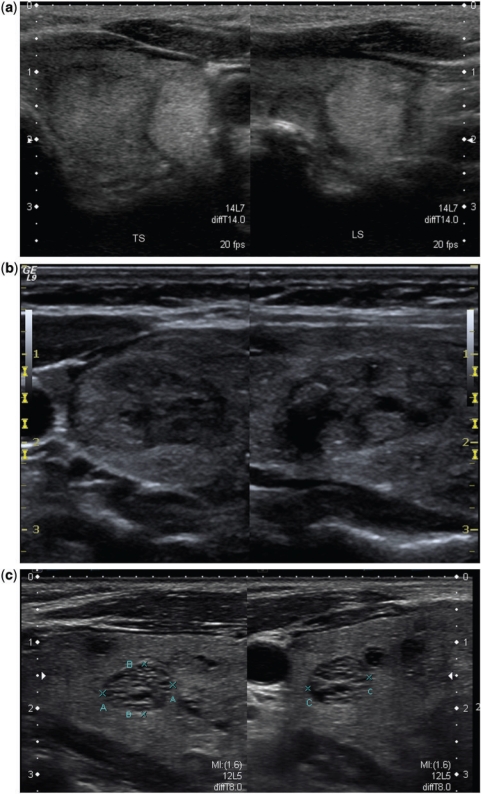
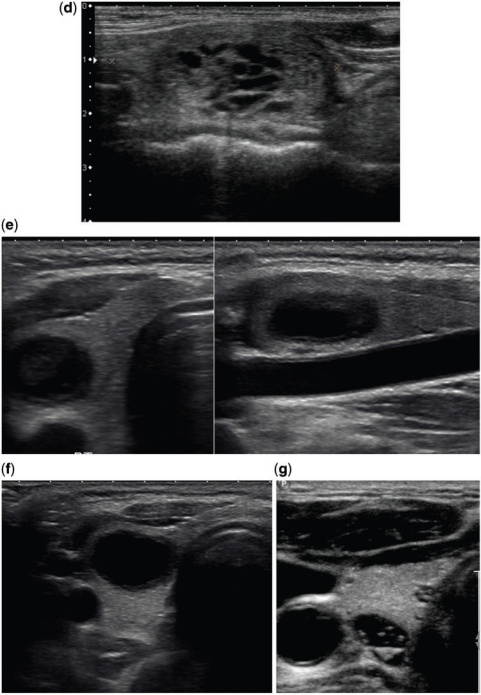
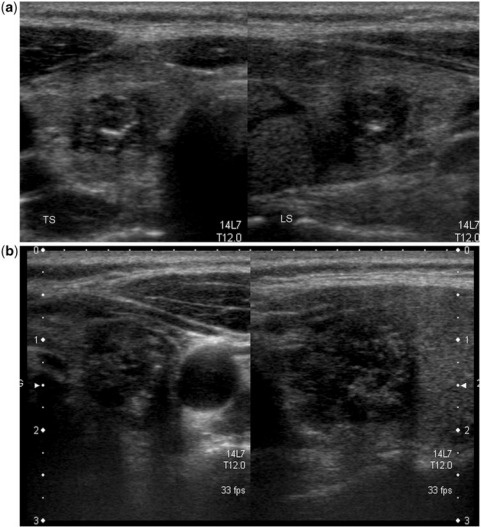
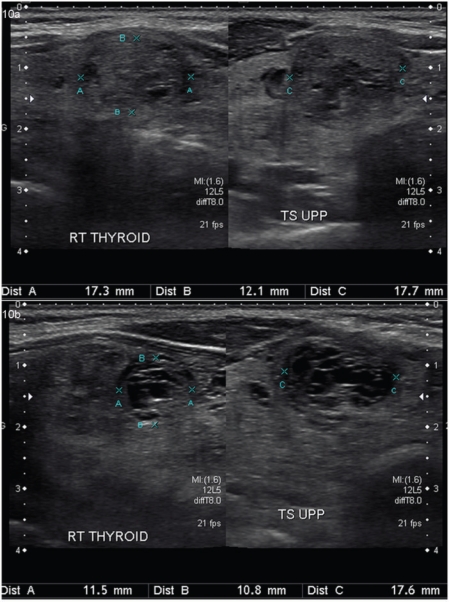
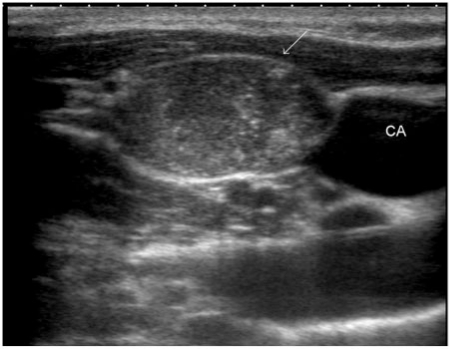
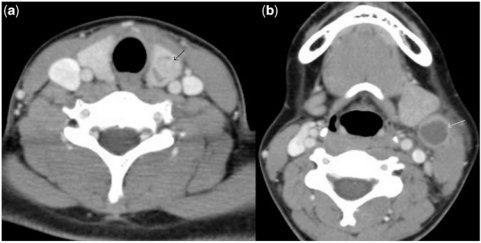
Replacing palpating fingers with an ultrasound (US) probe has resulted in an epidemic of thyroid nodules. Despite the high prevalence of thyroid nodules in the general population, thyroid malignancy is rare. Although no imaging modality can accurately predict the nature of every nodule, high-resolution US is the most sensitive, easily available and cost-effective diagnostic test available to detect thyroid nodules, measure their dimensions and identify their structure. The presence of calcifications, irregular spiculated outline, hypoechogenicity in a solid nodule, chaotic intranodular vascularity and an elongated shape are well-known US features of malignancy in thyroid nodules. Cervical lymph node metastasis and extrathyroidal extension of a thyroid nodule are highly specific for malignancy but seen infrequently. Spongiform nodules, purely or predominantly cystic nodules, nodules with well-defined hypoechoic halo and echogenic as well as isoechoic nodules are usually benign. None of the US characteristics have 100% accuracy in detecting or excluding malignancy. Fine-needle biopsy is currently the best triage test for pre-operative evaluation of a thyroid nodule. There is no significant difference in the risk for malignancy between palpable and non-palpable nodules and size is not a reliable indicator for their malignant potential. The best tool for risk stratification for malignancy in thyroid nodules is US and guided biopsy of nodules with suspicious imaging features. This is especially relevant in patients with multinodular goitre.
Figures


Similar articles
-
Partially cystic thyroid nodules in ultrasound-guided fine needle aspiration: Prevalence of thyroid carcinoma and ultrasound features.Medicine (Baltimore). 2017 Nov;96(46):e8689. doi: 10.1097/MD.0000000000008689. Medicine (Baltimore). 2017. PMID: 29145304 Free PMC article.
-
Ultrasound-guided thyroid nodule biopsy: outcomes and correlation with imaging features.Clin Imaging. 2015 Mar-Apr;39(2):200-6. doi: 10.1016/j.clinimag.2014.10.019. Epub 2014 Nov 7. Clin Imaging. 2015. PMID: 25475702
-
Malignancy risk stratification in thyroid nodules with nondiagnostic results at cytologic examination: combination of thyroid imaging reporting and data system and the Bethesda System.Radiology. 2015 Jan;274(1):287-95. doi: 10.1148/radiol.14140359. Epub 2014 Aug 18. Radiology. 2015. PMID: 25133852
-
Current status of fine needle aspiration for thyroid nodules.Adv Surg. 2006;40:223-38. doi: 10.1016/j.yasu.2006.06.003. Adv Surg. 2006. PMID: 17163105 Review.
-
Role of thyroid ultrasound in the diagnostic evaluation of thyroid nodules.Best Pract Res Clin Endocrinol Metab. 2008 Dec;22(6):913-28. doi: 10.1016/j.beem.2008.09.016. Best Pract Res Clin Endocrinol Metab. 2008. PMID: 19041822 Review.
Cited by
-
Thyroid Hormones, Autoantibodies, Ultrasonography, and Clinical Parameters for Predicting Thyroid Cancer.Int J Endocrinol. 2016;2016:8215834. doi: 10.1155/2016/8215834. Epub 2016 May 19. Int J Endocrinol. 2016. PMID: 27313612 Free PMC article.
-
Diagnostic Value of AngioPLUS Microvascular Imaging in Thyroid Nodule Diagnosis Using Quantitative and Qualitative Vascularity Grading.Biomedicines. 2022 Jun 29;10(7):1554. doi: 10.3390/biomedicines10071554. Biomedicines. 2022. PMID: 35884858 Free PMC article.
-
Do intranodular macrocalcifications really play an important role in sonographic prediction of malignancy?Yonsei Med J. 2014 Sep;55(5):1450-1. doi: 10.3349/ymj.2014.55.5.1450. Yonsei Med J. 2014. PMID: 25048511 Free PMC article. No abstract available.
-
Challenges in Preoperative Diagnosis for Thyroid Nodules Classified as Follicular Lesions of Undetermined Significance or Follicular Neoplasms.J Korean Soc Radiol. 2025 Jan;86(1):127-128. doi: 10.3348/jksr.2025.0003. Epub 2025 Jan 23. J Korean Soc Radiol. 2025. PMID: 39958492 Free PMC article. No abstract available.
-
The Importance of the Thyroid Nodule Location in Determining the Risk of Malignancy: A Retrospective Study.Cureus. 2022 Sep 21;14(9):e29421. doi: 10.7759/cureus.29421. eCollection 2022 Sep. Cureus. 2022. PMID: 36299930 Free PMC article.
References
-
- Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and EuropeanThyroid Association Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules. Endocr Pract. 2010;16(Suppl 1):1–43. doi: 10.4158/10024.GL. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources