

Sildenafil prevents and reverses transverse-tubule remodeling and Ca(2+) handling dysfunction in right ventricle failure induced by pulmonary artery hypertension
- PMID: 22203744
- PMCID: PMC3266850
- DOI: 10.1161/HYPERTENSIONAHA.111.180968
Sildenafil prevents and reverses transverse-tubule remodeling and Ca(2+) handling dysfunction in right ventricle failure induced by pulmonary artery hypertension
Abstract
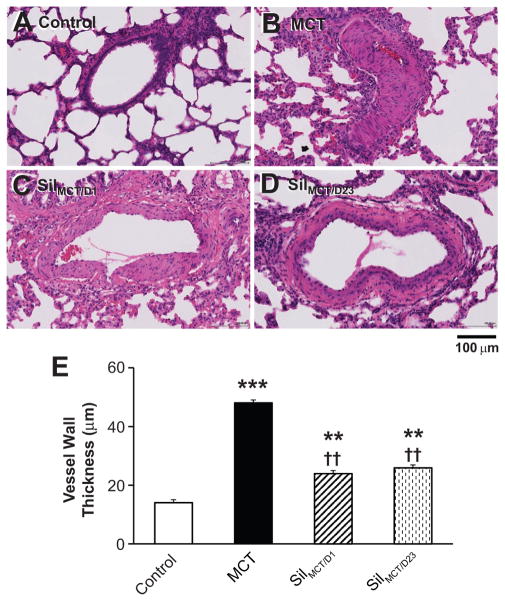
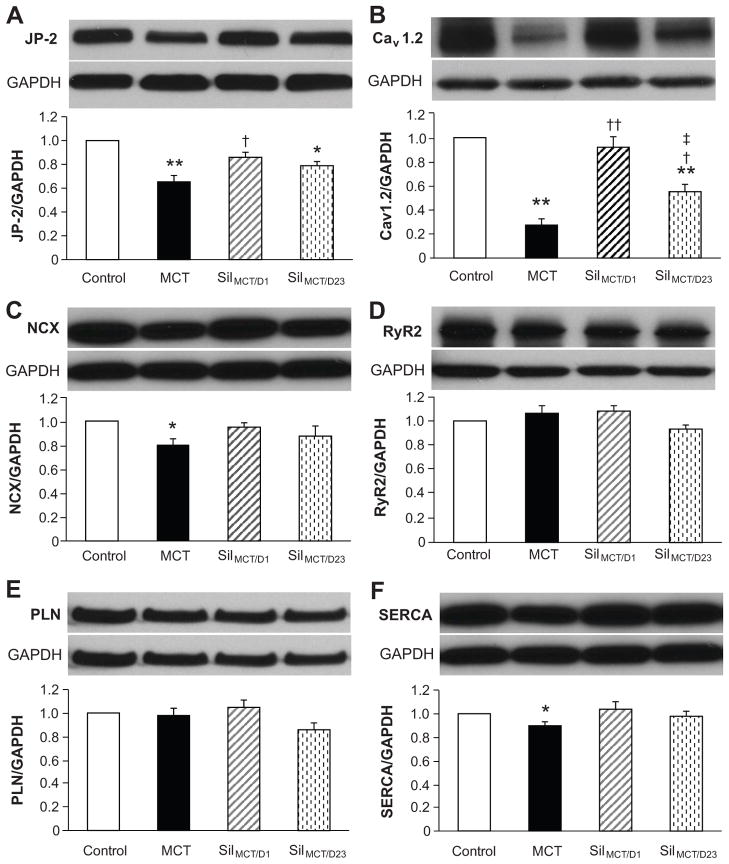
Right ventricular (RV) failure (RVF) is the main cause of death in patients with pulmonary artery hypertension (PAH). Sildenafil, a phosphodiesterase type 5 inhibitor, was approved recently for treatment of PAH patients. However, the mechanisms underlying RV contractile malfunction and the benefits of sildenafil on RV function are not well understood. We aimed to investigate the following: (1) the ultrastructural and excitation-contraction coupling alterations underlying PAH-induced RVF; (2) whether the ultrastructural changes are reversible; and (3) the mechanisms underlying the therapeutic benefits of sildenafil in PAH-RVF. We used a single injection of monocrotaline in Wistar rats to induce pulmonary vascular proliferation, which led to PAH and RVF. RV myocytes displayed severe transverse (T)-tubule loss and disorganization, as well as blunted and dys-synchronous sarcoplasmic reticulum Ca(2+) release. Sildenafil prevented and reversed the monocrotaline-induced PAH and LV filling impairment. Early intervention with sildenafil prevented RV hypertrophy and the development of RVF, T-tubule remodeling, and Ca(2+) handling dysfunction. Although late treatment with sildenafil did not reverse RV hypertrophy in animals with established RVF, RV systolic function was improved. Furthermore, late intervention partially reversed both the impairment of myocyte T-tubule integrity and Ca(2+) handling protein and sarcoplasmic reticulum Ca(2+) release function in monocrotaline-treated rats. In conclusion, PAH-induced increase in RV afterload causes severe T-tubule remodeling and Ca(2+) handling dysfunction in RV myocytes, leading to RV contractile failure. Sildenafil prevents and partially reverses ultrastructural, molecular, and functional remodeling of failing RV myocytes. Reversal of pathological T-tubule remodeling, although incomplete, is achievable without the regression of RV hypertrophy.
Conflict of interest statement
No conflict of interest to be disclosed.
Figures




References
-
- Heinzel FR, Bito V, Biesmans L, Wu M, Detre E, von Wegner F, Claus P, Dymarkowski S, Maes F, Bogaert J, Rademakers F, D’Hooge J, Sipido K. Remodeling of t-tubules and reduced synchrony of Ca2+ release in myocytes from chronically ischemic myocardium. Circ Res. 2008;102:338–346. - PubMed
-
- Balijepalli RC, Lokuta AJ, Maertz NA, Buck JM, Haworth RA, Valdivia HH, Kamp TJ. Depletion of t-tubules and specific subcellular changes in sarcolemmal proteins in tachycardia-induced heart failure. Cardiovasc Res. 2003;59:67–77. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
