

Ebola haemorrhagic fever outbreak in Masindi District, Uganda: outbreak description and lessons learned
- PMID: 22204600
- PMCID: PMC3276451
- DOI: 10.1186/1471-2334-11-357
Ebola haemorrhagic fever outbreak in Masindi District, Uganda: outbreak description and lessons learned
Abstract
Background: Ebola haemorrhagic fever (EHF) is infamous for its high case-fatality proportion (CFP) and the ease with which it spreads among contacts of the diseased. We describe the course of the EHF outbreak in Masindi, Uganda, in the year 2000, and report on response activities.
Methods: We analysed surveillance records, hospital statistics, and our own observations during response activities. We used Fisher's exact tests for differences in proportions, t-tests for differences in means, and logistic regression for multivariable analysis.
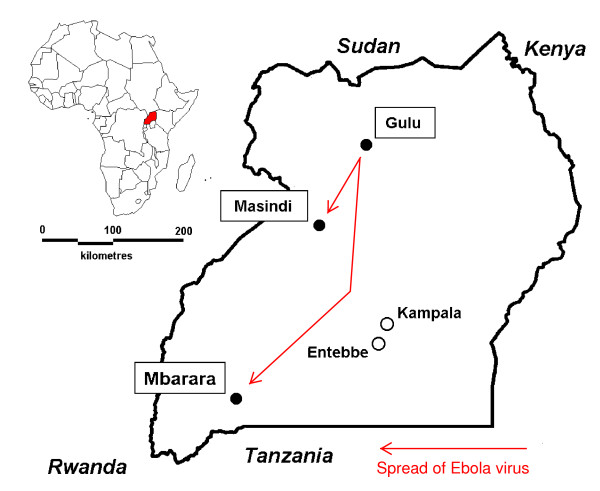
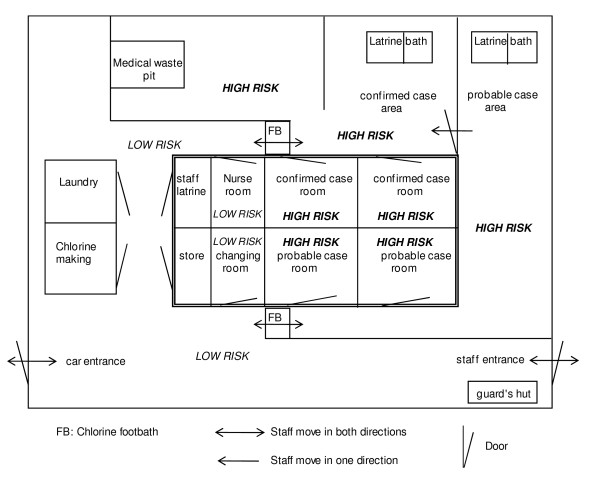
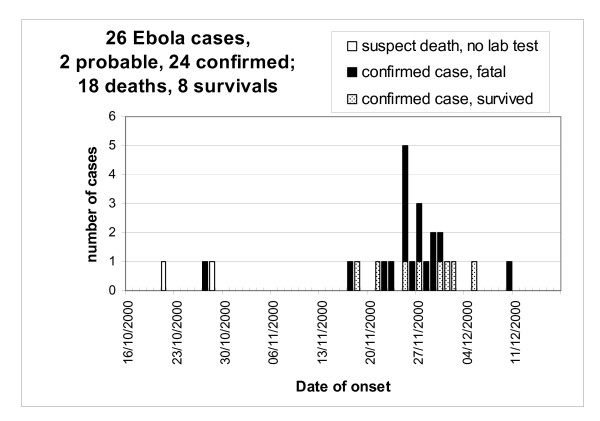
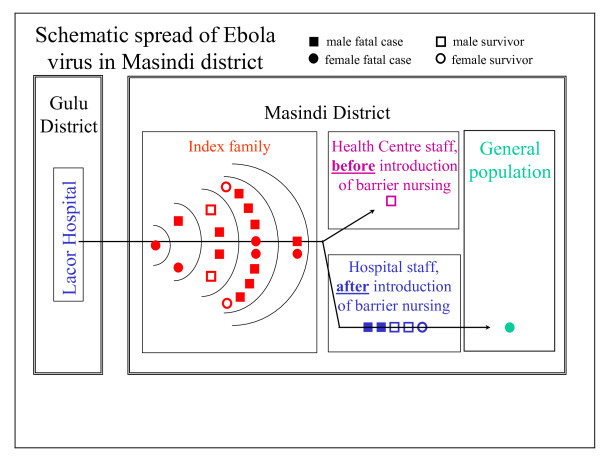
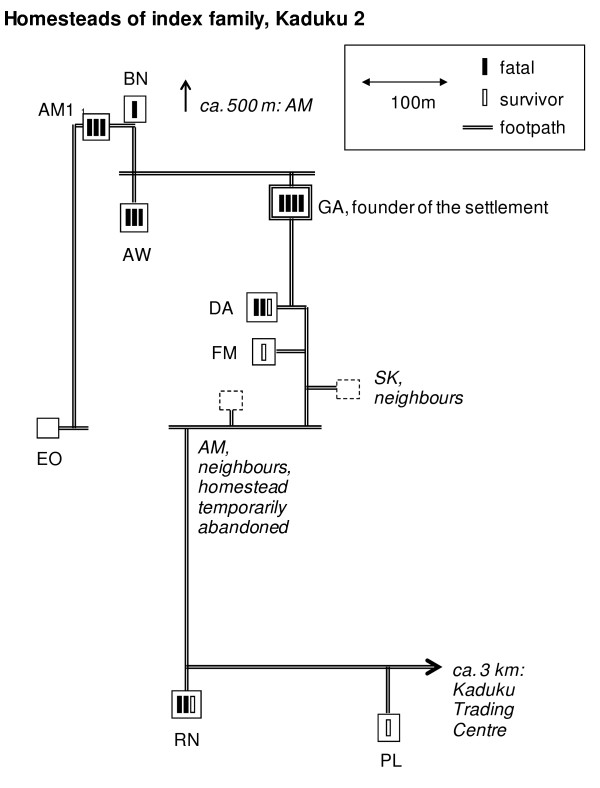
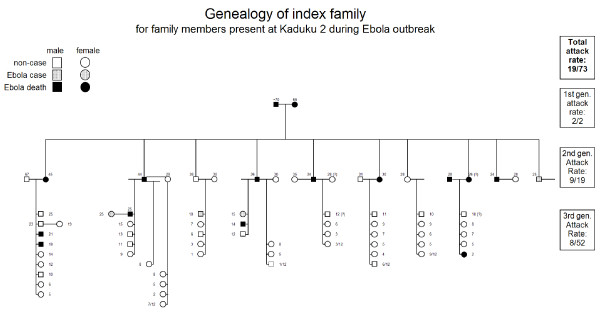
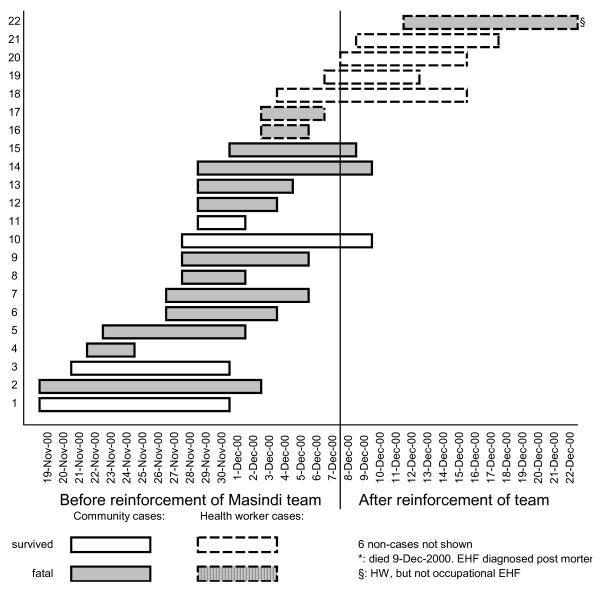
Results: The response to the outbreak consisted of surveillance, case management, logistics and public mobilisation. Twenty-six EHF cases (24 laboratory confirmed, two probable) occurred between October 21st and December 22nd, 2000. CFP was 69% (18/26). Nosocomial transmission to the index case occurred in Lacor hospital in Gulu, outside the Ebola ward. After returning home to Masindi district the index case became the origin of a transmission chain within her own extended family (18 further cases), from index family members to health care workers (HCWs, 6 cases), and from HCWs to their household contacts (1 case). Five out of six occupational cases of EHF in HCWs occurred after the introduction of barrier nursing, probably due to breaches of barrier nursing principles. CFP was initially very high (76%) but decreased (20%) due to better case management after reinforcing the response team. The mobilisation of the community for the response efforts was challenging at the beginning, when fear, panic and mistrust had to be countered by the response team.
Conclusions: Large scale transmission in the community beyond the index family was prevented by early case identification and isolation as well as quarantine imposed by the community. The high number of occupational EHF after implementing barrier nursing points at the need to strengthen training and supervision of local HCWs. The difference in CFP before and after reinforcing the response team together with observations on the ward suggest a critical role for intensive supportive treatment. Collecting high quality clinical data is a priority for future outbreaks in order to identify the best possible FHF treatment regime under field conditions.
Figures
References
-
- WHO. Outbreak of Ebola haemorrhagic fever, Uganda, August 2000-January 2001. Wkly Epidemiol Rec. 2001;76(6):41–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
