

Complement activating antibodies to myelin oligodendrocyte glycoprotein in neuromyelitis optica and related disorders
- PMID: 22204662
- PMCID: PMC3278385
- DOI: 10.1186/1742-2094-8-184
Complement activating antibodies to myelin oligodendrocyte glycoprotein in neuromyelitis optica and related disorders
Abstract
Background: Serum autoantibodies against the water channel aquaporin-4 (AQP4) are important diagnostic biomarkers and pathogenic factors for neuromyelitis optica (NMO). However, AQP4-IgG are absent in 5-40% of all NMO patients and the target of the autoimmune response in these patients is unknown. Since recent studies indicate that autoimmune responses to myelin oligodendrocyte glycoprotein (MOG) can induce an NMO-like disease in experimental animal models, we speculate that MOG might be an autoantigen in AQP4-IgG seronegative NMO. Although high-titer autoantibodies to human native MOG were mainly detected in a subgroup of pediatric acute disseminated encephalomyelitis (ADEM) and multiple sclerosis (MS) patients, their role in NMO and High-risk NMO (HR-NMO; recurrent optic neuritis-rON or longitudinally extensive transverse myelitis-LETM) remains unresolved.
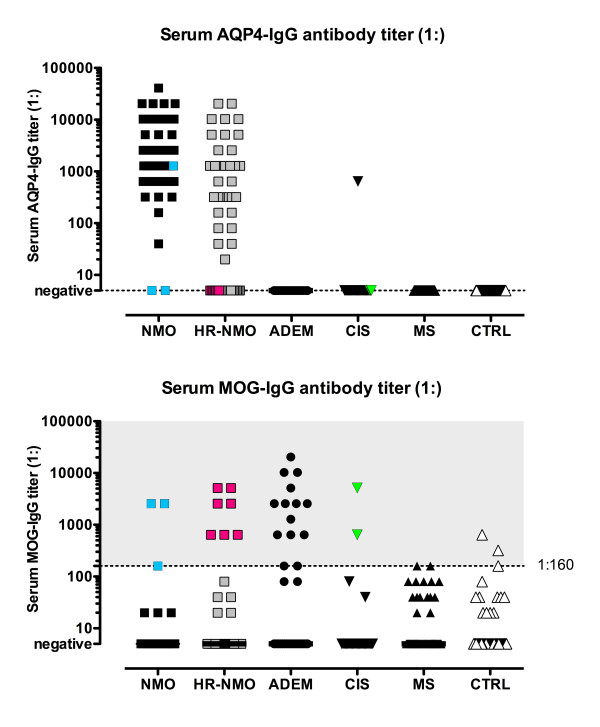
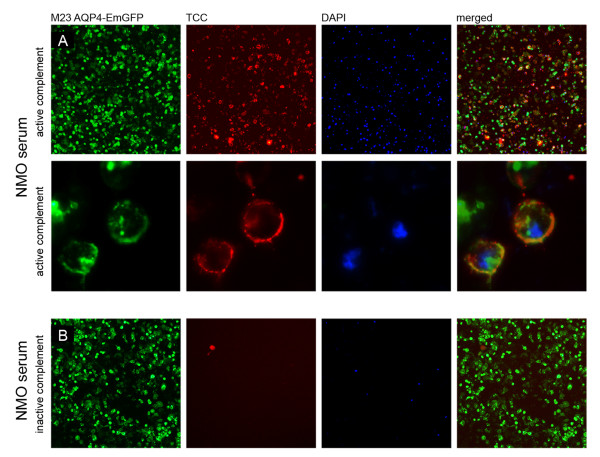
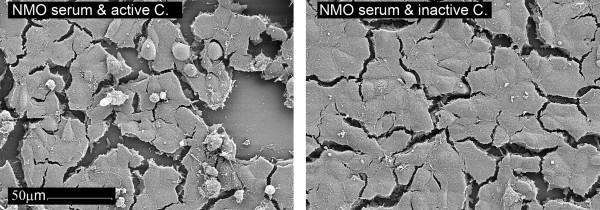
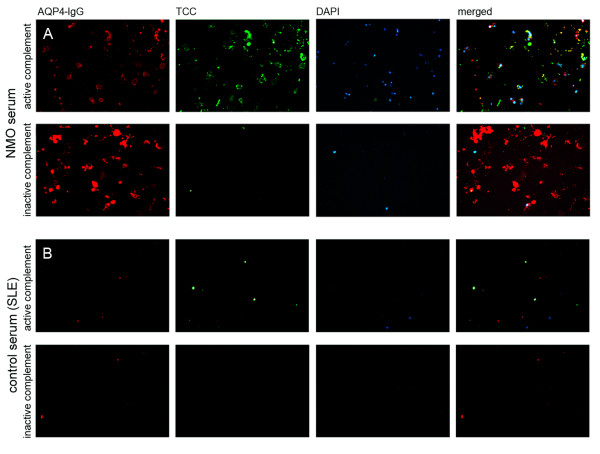
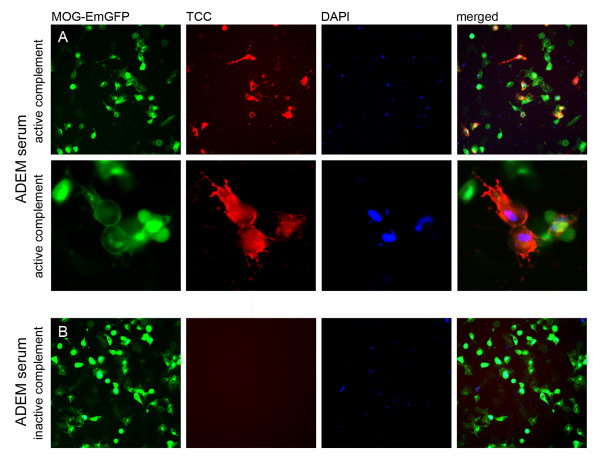
Results: We analyzed patients with definite NMO (n = 45), HR-NMO (n = 53), ADEM (n = 33), clinically isolated syndromes presenting with myelitis or optic neuritis (CIS, n = 32), MS (n = 71) and controls (n = 101; 24 other neurological diseases-OND, 27 systemic lupus erythematosus-SLE and 50 healthy subjects) for serum IgG to MOG and AQP4. Furthermore, we investigated whether these antibodies can mediate complement dependent cytotoxicity (CDC). AQP4-IgG was found in patients with NMO (n = 43, 96%), HR-NMO (n = 32, 60%) and in one CIS patient (3%), but was absent in ADEM, MS and controls. High-titer MOG-IgG was found in patients with ADEM (n = 14, 42%), NMO (n = 3, 7%), HR-NMO (n = 7, 13%, 5 rON and 2 LETM), CIS (n = 2, 6%), MS (n = 2, 3%) and controls (n = 3, 3%, two SLE and one OND). Two of the three MOG-IgG positive NMO patients and all seven MOG-IgG positive HR-NMO patients were negative for AQP4-IgG. Thus, MOG-IgG were found in both AQP4-IgG seronegative NMO patients and seven of 21 (33%) AQP4-IgG negative HR-NMO patients. Antibodies to MOG and AQP4 were predominantly of the IgG1 subtype, and were able to mediate CDC at high-titer levels.
Conclusions: We could show for the first time that a subset of AQP4-IgG seronegative patients with NMO and HR-NMO exhibit a MOG-IgG mediated immune response, whereas MOG is not a target antigen in cases with an AQP4-directed humoral immune response.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
