

Multiplex immunoassays of peptide hormones extracted from formalin-fixed, paraffin-embedded tissue accurately subclassify pituitary adenomas
- PMID: 22205691
- PMCID: PMC4123741
- DOI: 10.1373/clinchem.2011.170613
Multiplex immunoassays of peptide hormones extracted from formalin-fixed, paraffin-embedded tissue accurately subclassify pituitary adenomas
Abstract
Background: The current gold standard for diagnostic classification of many solid-tissue neoplasms is immunohistochemistry (IHC) performed on formalin-fixed, paraffin-embedded (FFPE) tissue. Although IHC is commonly used, there remain important issues related to preanalytic variability, nonstandard methods, and operator bias that may contribute to clinically significant error. To increase the quantitative accuracy and reliability of FFPE tissue-based diagnosis, we sought to develop a clinical proteomic method to characterize protein expression in pathologic tissue samples rapidly and quantitatively.
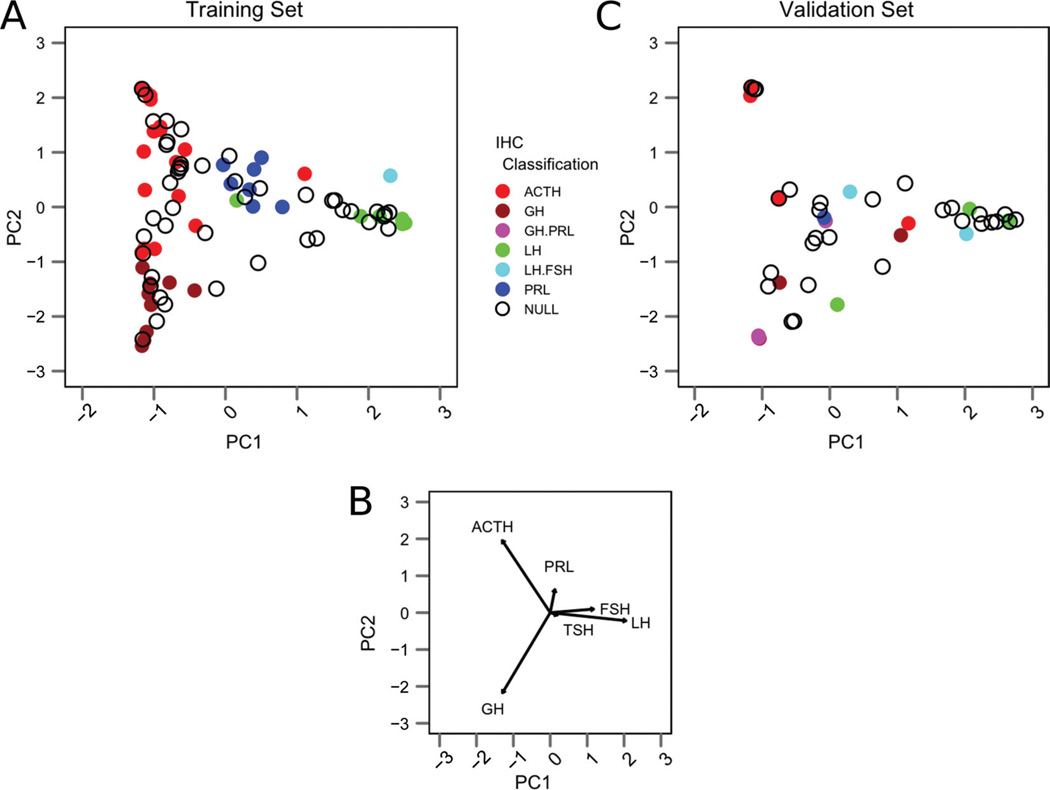
Methods: We subclassified FFPE tissue from 136 clinical pituitary adenoma samples according to hormone translation with IHC and then extracted tissue proteins and quantified pituitary hormones with multiplex bead-based immunoassays. Hormone concentrations were normalized and compared across diagnostic groups. We developed a quantitative classification scheme for pituitary adenomas on archived samples and validated it on prospectively collected clinical samples.
Results: The most abundant relative hormone concentrations differentiated sensitively and specifically between IHC-classified hormone-expressing adenoma types, correctly predicting IHC-positive diagnoses in 85% of cases overall, with discrepancies found only in cases of clinically nonfunctioning adenomas. Several adenomas with clinically relevant hormone-expressing phenotypes were identified with this assay yet called "null" by IHC, suggesting that multiplex immunoassays may be more sensitive than IHC for detecting clinically meaningful protein expression.
Conclusions: Multiplex immunoassays performed on FFPE tissue extracts can provide diagnostically relevant information and may exceed the performance of IHC in classifying some pituitary neoplasms. This technique is simple, largely amenable to automation, and likely applicable to other diagnostic problems in molecular pathology.
Conflict of interest statement
Figures



Similar articles
-
The Role of T-box Transcription Factor in a Pituitary Adenoma Diagnostic Algorithm.Arch Pathol Lab Med. 2021 May 1;145(5):592-598. doi: 10.5858/arpa.2020-0091-OA. Arch Pathol Lab Med. 2021. PMID: 32991684
-
Steroidogenic Factor 1, Pit-1, and Adrenocorticotropic Hormone: A Rational Starting Place for the Immunohistochemical Characterization of Pituitary Adenoma.Arch Pathol Lab Med. 2017 Jan;141(1):104-112. doi: 10.5858/arpa.2016-0082-OA. Epub 2016 May 26. Arch Pathol Lab Med. 2017. PMID: 27227698
-
A gene-protein assay for human epidermal growth factor receptor 2 (HER2): brightfield tricolor visualization of HER2 protein, the HER2 gene, and chromosome 17 centromere (CEN17) in formalin-fixed, paraffin-embedded breast cancer tissue sections.Diagn Pathol. 2012 May 30;7:60. doi: 10.1186/1746-1596-7-60. Diagn Pathol. 2012. PMID: 22647525 Free PMC article.
-
Contributions of immunohistochemistry and in situ hybridization to the functional analysis of pituitary adenomas.J Histochem Cytochem. 2000 Apr;48(4):445-58. doi: 10.1177/002215540004800401. J Histochem Cytochem. 2000. PMID: 10727285 Review.
-
Complete solubilization of formalin-fixed, paraffin-embedded tissue may improve proteomic studies.Proteomics Clin Appl. 2013 Apr;7(3-4):264-72. doi: 10.1002/prca.201200031. Epub 2013 Mar 6. Proteomics Clin Appl. 2013. PMID: 23339100 Free PMC article. Review.
Cited by
-
Evaluation of Protein Profiles From Treated Xenograft Tumor Models Identifies an Antibody Panel for Formalin-fixed and Paraffin-embedded (FFPE) Tissue Analysis by Reverse Phase Protein Arrays (RPPA).Mol Cell Proteomics. 2015 Oct;14(10):2775-85. doi: 10.1074/mcp.O114.045542. Epub 2015 Jun 23. Mol Cell Proteomics. 2015. PMID: 26106084 Free PMC article.
-
Research advances on the immune research and prospect of immunotherapy in pituitary adenomas.World J Surg Oncol. 2021 Jun 5;19(1):162. doi: 10.1186/s12957-021-02272-9. World J Surg Oncol. 2021. PMID: 34090476 Free PMC article. Review.
-
Potential biomarkers of miRNA in non-functional pituitary adenomas.World J Surg Oncol. 2021 Sep 9;19(1):270. doi: 10.1186/s12957-021-02383-3. World J Surg Oncol. 2021. PMID: 34503538 Free PMC article.
-
A Sex-Dependent, Tropic Role for Leptin in the Somatotrope as a Regulator of POU1F1 and POU1F1-Dependent Hormones.Endocrinology. 2016 Oct;157(10):3958-3971. doi: 10.1210/en.2016-1472. Epub 2016 Aug 29. Endocrinology. 2016. PMID: 27571135 Free PMC article.
-
Heterogeneity analysis of the proteomes in clinically nonfunctional pituitary adenomas.BMC Med Genomics. 2014 Dec 24;7:69. doi: 10.1186/s12920-014-0069-6. BMC Med Genomics. 2014. PMID: 25539738 Free PMC article.
References
-
- Oien K. Pathologic evaluation of unknown primary cancer. Semin Oncol. 2009;36:8–37. - PubMed
-
- Carlson J, Fletcher C. Immunohistochemistry for beta-catenin in the differential diagnosis of spindle cell lesions: analysis of a series and review of the literature. Histopathology. 2007;51:509–514. - PubMed
-
- Gown A. Unmasking the mysteries of antigen or epitope retrieval and formalin fixation. Am J Clin Pathol. 2004;121:172–174. - PubMed
-
- Hede K. Breast cancer testing scandal shines spotlight on black box of clinical laboratory testing. J Natl Cancer Inst. 2008;100:836–844. - PubMed
-
- Camp RL, Chung GG, Rimm DL. Automated subcellular localization and quantification of protein expression in tissue microarrays. Nat Med. 2002;8:1323–1327. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
