

Recovery after spinal cord infarcts: long-term outcome in 115 patients
- PMID: 22205760
- PMCID: PMC3466672
- DOI: 10.1212/WNL.0b013e31823efc93
Recovery after spinal cord infarcts: long-term outcome in 115 patients
Abstract
Objective: To investigate the long-term outcome of patients with spinal cord infarct (SCI) and identify prognostic predictors.
Methods: We reviewed 115 patients with SCI treated between 1990 and 2007. Severity of impairment was defined using the American Spinal Injury Association (ASIA) scoring. Functional outcome endpoints were ambulatory status, need for bladder catheterization, and pain.
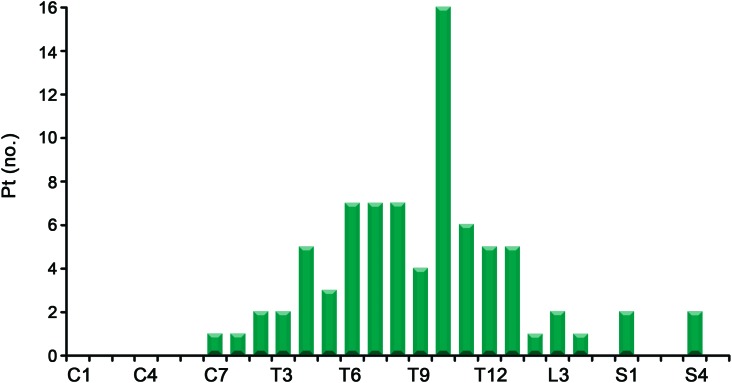
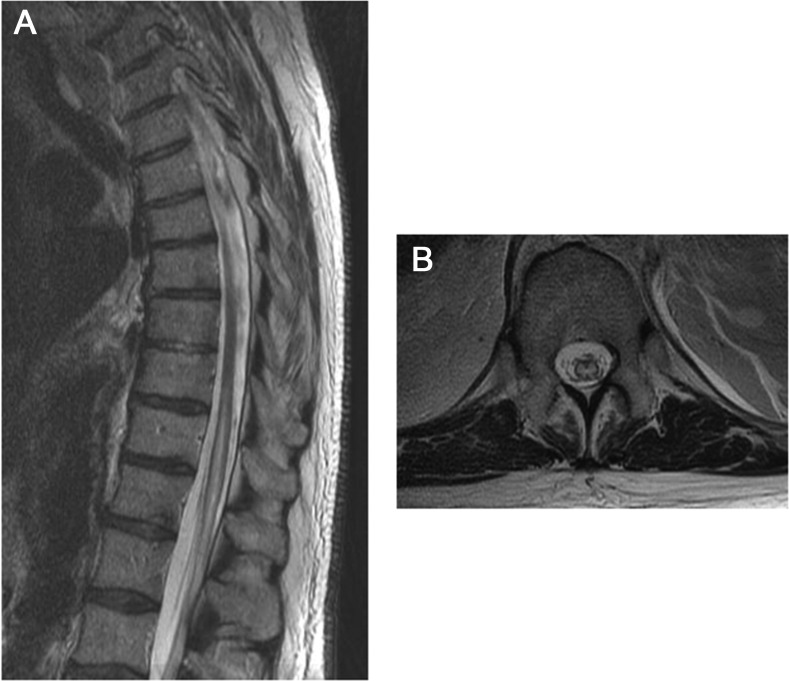
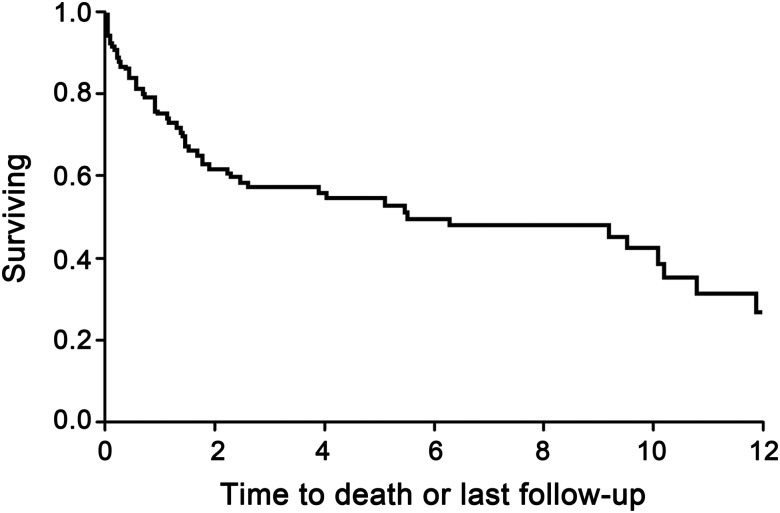
Results: Mean age was 64 years; 72 (62.6%) patients were men. A total of 45% of infarcts were perioperative (69% aortic surgeries). A total of 68% reached maximal deficit within 1 hour (mean = 5 hours). Impairment at nadir was ASIA A 23%, B 26%, C 14%, and D 37%. A total of 75/93 (81%) patients studied with MRI had cord signal abnormality. At nadir, 81% required wheelchair, 86% required catheterization, and 32% had pain. At last follow-up (mean = 3 years), 23% had died. Among survivors, 42% required a wheelchair, 54% required catheterization, and 29% had pain upon last follow-up. Of 74 patients using a wheelchair at hospital dismissal, 41% were walking by final follow-up. Of 83 patients catheterized at dismissal, 33% were catheter-free at last follow-up. Older age (p < 0.0001), increased severity of impairment at nadir (p = 0.02), and peripheral vascular disease (p = 0.003) were independent risk factors for mortality. Severe impairment (ASIA A/B) at nadir predicted wheelchair use (p < 0.0001) and bladder catheterization (p < 0.0001) at last follow-up.
Conclusions: Gradual improvement in not uncommon after spinal cord infarction and it may continue long after hospital dismissal. While severe impairment at nadir is the strongest predictor of poor functional outcome, meaningful recovery is also possible in a substantial minority of these patients.
Figures
References
-
- Sandson TA, Friedman JH. Spinal cord infarction: report of 8 cases and review of the literature. Medicine 1989;68:282–292 - PubMed
-
- de Seze J, Stojkovic T, Breteau G, et al. Acute myelopathies: clinical, laboratory and outcome profiles in 79 cases. Brain 2001;124:1509–1521 - PubMed
-
- Novy J, Carruzzo A, Maeder P, Bogousslavsky J. Spinal cord ischemia: clinical and imaging patterns, pathogenesis, and outcomes in 27 patients. Arch Neurol 2006;63:1113–1120 - PubMed
-
- Salvador de la Barrera S, Barca-Buyo A, Montoto-Marques A, et al. Spinal cord infarction: prognosis and recovery in a series of 36 patients. Spinal Cord 2001;39:520–525 - PubMed
-
- Cheshire WP, Santos CC, Massey EW, Howard JF., Jr Spinal cord infarction: etiology and outcome. Neurology 1996;47:321–330 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical