

Sex-specific immunization for sexually transmitted infections such as human papillomavirus: insights from mathematical models
- PMID: 22205887
- PMCID: PMC3243713
- DOI: 10.1371/journal.pmed.1001147
Sex-specific immunization for sexually transmitted infections such as human papillomavirus: insights from mathematical models
Abstract
Background: Sex-specific differences regarding the transmissibility and the course of infection are the rule rather than the exception in the epidemiology of sexually transmitted infections (STIs). Human papillomavirus (HPV) provides an example: disease outcomes differ between men and women, as does the potential for transmission to the opposite sex. HPV vaccination of preadolescent girls was recently introduced in many countries, and inclusion of boys in the vaccination programs is being discussed. Here, we address the question of whether vaccinating females only, males only, or both sexes is the most effective strategy to reduce the population prevalence of an STI like HPV.
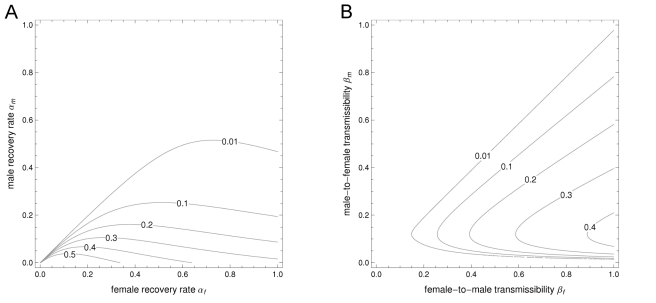
Methods and findings: We use a range of two-sex transmission models with varying detail to identify general criteria for allocating a prophylactic vaccine between both sexes. The most effective reduction in the population prevalence of infection is always achieved by single-sex vaccination; vaccinating the sex with the highest prevaccine prevalence is the preferred strategy in most circumstances. Exceptions arise only when the higher prevaccine prevalence is due to a substantially lower rate of natural immunity, or when natural immunity is lifelong, and a prolonged duration of infectiousness coincides with increased transmissibility. Predictions from simple models were confirmed in simulations based on an elaborate HPV transmission model. Our analysis suggests that relatively inefficient genital transmission from males to females might render male vaccination more effective in reducing overall infection levels. However, most existing HPV vaccination programs have achieved sufficient coverage to continue with female-only vaccination.
Conclusions: Increasing vaccine uptake among preadolescent girls is more effective in reducing HPV infection than including boys in existing vaccination programs. As a rule, directing prophylactic immunization at the sex with the highest prevaccine prevalence results in the largest reduction of the population prevalence.
Conflict of interest statement
CJLMM and JB have received unrestricted research grants from GSK. JB also acted as research consultant for Sanofi Pasteur MSD. MK acted as a research consultant for Sanofi Pasteur MSD and for GSK. The other authors have declared no competing interests.
Figures



Similar articles
-
Potential effectiveness of prophylactic HPV immunization for men who have sex with men in the Netherlands: A multi-model approach.PLoS Med. 2019 Mar 4;16(3):e1002756. doi: 10.1371/journal.pmed.1002756. eCollection 2019 Mar. PLoS Med. 2019. PMID: 30830901 Free PMC article.
-
Assessing the cost-effectiveness of HPV vaccination strategies for adolescent girls and boys in the UK.BMC Infect Dis. 2019 Jun 24;19(1):552. doi: 10.1186/s12879-019-4108-y. BMC Infect Dis. 2019. PMID: 31234784 Free PMC article.
-
Quadrivalent Human Papillomavirus Vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP).MMWR Recomm Rep. 2007 Mar 23;56(RR-2):1-24. MMWR Recomm Rep. 2007. PMID: 17380109
-
[Experimental vaccines for sexually transmitted infections].Med Pregl. 2009 Jan-Feb;62(1-2):42-8. doi: 10.2298/mpns0902042j. Med Pregl. 2009. PMID: 19514600 Review. Serbian.
-
Moving forward: human papillomavirus vaccination and the prevention of cervical cancer.J Womens Health (Larchmt). 2007 Nov;16(9):1258-68. doi: 10.1089/jwh.2007.0493. J Womens Health (Larchmt). 2007. PMID: 18001182 Review.
Cited by
-
Impact of vaccination on 14 high-risk HPV type infections: a mathematical modelling approach.PLoS One. 2013 Aug 29;8(8):e72088. doi: 10.1371/journal.pone.0072088. eCollection 2013. PLoS One. 2013. PMID: 24009669 Free PMC article.
-
Genital Chlamydia trachomatis: understanding the roles of innate and adaptive immunity in vaccine research.Clin Microbiol Rev. 2014 Apr;27(2):346-70. doi: 10.1128/CMR.00105-13. Clin Microbiol Rev. 2014. PMID: 24696438 Free PMC article. Review.
-
Incremental benefits of male HPV vaccination: accounting for inequality in population uptake.PLoS One. 2014 Aug 4;9(8):e101048. doi: 10.1371/journal.pone.0101048. eCollection 2014. PLoS One. 2014. PMID: 25089637 Free PMC article.
-
Population-level impact and herd effects following human papillomavirus vaccination programmes: a systematic review and meta-analysis.Lancet Infect Dis. 2015 May;15(5):565-80. doi: 10.1016/S1473-3099(14)71073-4. Epub 2015 Mar 3. Lancet Infect Dis. 2015. PMID: 25744474 Free PMC article.
-
Extending the Human Papillomavirus Vaccination Programme to Include Males in High-Income Countries: A Systematic Review of the Cost-Effectiveness Studies.Clin Drug Investig. 2015 Aug;35(8):471-85. doi: 10.1007/s40261-015-0308-4. Clin Drug Investig. 2015. PMID: 26187455
References
-
- Hethcote HW, Yorke JA. Gonorrhea: transmission dynamics and control. Lecture notes in biomathematics 56. Berlin: Springer-Verlag; 1984. 105 Available: http://www.math.uiowa.edu/ftp/hethcote/lnb56.pdf. Accessed 12 August 2011.
-
- Kretzschmar M, van Duynhoven YT, Severijnen AJ. Modeling prevention strategies for gonorrhea and chlamydia using stochastic network simulations. Am J Epidemiol. 1996;144:306–317. - PubMed
-
- Gray RT, Beagley KW, Timms P, Wilson DP. Modeling the impact of potential vaccines on epidemics of sexually transmitted Chlamydia trachomatis infection. J Infect Dis. 2009;199:1680–1688. - PubMed
-
- Williams BG, Lloyd-Smith JO, Gouws E, Hankins C, Getz WM, et al. The potential impact of male circumcision on HIV in Sub-Saharan Africa. PLoS Med. 2006;3:e262. doi: 10.1371/journal.pmed.0030262. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
