

Estimating loss to follow-up in HIV-infected patients on antiretroviral therapy: the effect of the competing risk of death in Zambia and Switzerland
- PMID: 22205933
- PMCID: PMC3242760
- DOI: 10.1371/journal.pone.0027919
Estimating loss to follow-up in HIV-infected patients on antiretroviral therapy: the effect of the competing risk of death in Zambia and Switzerland
Abstract
Background: Loss to follow-up (LTFU) is common in antiretroviral therapy (ART) programmes. Mortality is a competing risk (CR) for LTFU; however, it is often overlooked in cohort analyses. We examined how the CR of death affected LTFU estimates in Zambia and Switzerland.
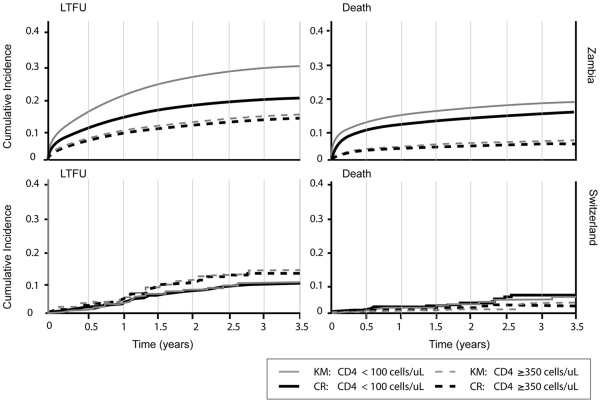
Methods and findings: HIV-infected patients aged ≥18 years who started ART 2004-2008 in observational cohorts in Zambia and Switzerland were included. We compared standard Kaplan-Meier curves with CR cumulative incidence. We calculated hazard ratios for LTFU across CD4 cell count strata using cause-specific Cox models, or Fine and Gray subdistribution models, adjusting for age, gender, body mass index and clinical stage. 89,339 patients from Zambia and 1,860 patients from Switzerland were included. 12,237 patients (13.7%) in Zambia and 129 patients (6.9%) in Switzerland were LTFU and 8,498 (9.5%) and 29 patients (1.6%), respectively, died. In Zambia, the probability of LTFU was overestimated in Kaplan-Meier curves: estimates at 3.5 years were 29.3% for patients starting ART with CD4 cells <100 cells/µl and 15.4% among patients starting with ≥ 350 cells/µL. The estimates from CR cumulative incidence were 22.9% and 13.6%, respectively. Little difference was found between naïve and CR analyses in Switzerland since only few patients died. The results from Cox and Fine and Gray models were similar: in Zambia the risk of loss to follow-up and death increased with decreasing CD4 counts at the start of ART, whereas in Switzerland there was a trend in the opposite direction, with patients with higher CD4 cell counts more likely to be lost to follow-up.
Conclusions: In ART programmes in low-income settings the competing risk of death can substantially bias standard analyses of LTFU. The CD4 cell count and other prognostic factors may be differentially associated with LTFU in low-income and high-income settings.
Conflict of interest statement
Figures
References
-
- Ledergerber B, von Overbeck J, Egger M, Luthy R. The Swiss HIV Cohort Study: rationale, organization and selected baseline characteristics. Soz Praventivmed. 1994;39:387–394. - PubMed
-
- Schoeni-Affolter F, Ledergerber B, Rickenbach M, Rudin C, Gunthard HF, et al. Cohort profile: the Swiss HIV Cohort study. Int J Epidemiol. 2010;39:1179–1189. - PubMed
-
- Hessol NA, Schneider M, Greenblatt RM, Bacon M, Barranday Y, et al. Retention of women enrolled in a prospective study of human immunodeficiency virus infection: impact of race, unstable housing, and use of human immunodeficiency virus therapy. Am J Epidemiol. 2001;154:563–573. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
