

Surgery of skeletal metastases in 306 patients with prostate cancer
- PMID: 22206449
- PMCID: PMC3278661
- DOI: 10.3109/17453674.2011.645197
Surgery of skeletal metastases in 306 patients with prostate cancer
Abstract
Purpose: Skeletal metastases are common in patients with prostate cancer, and they can be a source of considerable morbidity. We analyzed patient survival after surgery for skeletal metastases and identified risk factors for reoperation and complications.
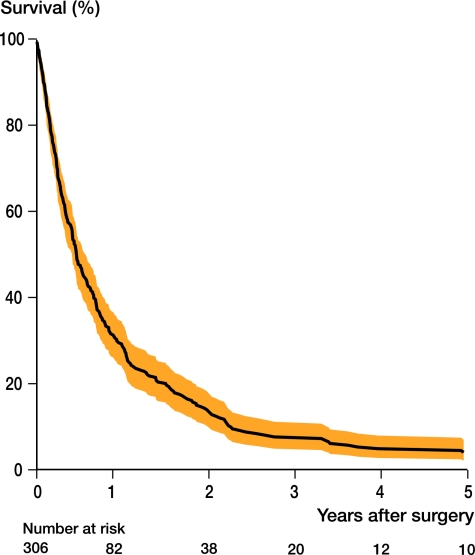
Patients and methods: This study included 306 patients with prostate cancer operated for skeletal metastases during 1989-2010. Kaplan-Meier analysis was used to calculate survival. Cox multiple regression analysis was performed to study risk factors, and results were expressed as hazard ratios (HRs).
Results: The median age at surgery was 72 (49-94) years. The median survival after surgery was 0.5 (0-16) years. The cumulative 1-, 2-, and 3-year survival after surgery was 29% (95% CI: 24-34), 14% (10-18), and 8% (5-11). Age over 70 years (HR 1.4), generalized metastases (HR 2.4), and multiple skeletal metastases (HR 2.3) resulted in an increased risk of death after surgery. Patients with lesions in the humerus (HR 0.6) had a lower death rate. The reoperation rate was 9% (n = 31). The reasons for reoperation were deep wound infection (n = 10), hematoma (n = 7), material (implant) failure (n = 3), wound dehiscence (n = 3), increasing neurological symptoms (n = 2), prosthetic dislocation (n = 2), and others (n = 4).
Interpretation: This study involves the largest reported cohort of patients operated for skeletal lesions from prostate cancer. Our survival data and analysis of predictors for survival help to set appropriate expectations for the patients, families, and medical staff.
Figures
References
-
- Atanasiu JP, Badatcheff F, Pidhorz L. Metastatic lesions of the cervical spine. A retrospective analysis of 20 cases. Spine. 1993;18:1279–84. - PubMed
-
- Bauer HC, Wedin R. Survival after surgery for spinal and extremity metastases. Prognostication in 241 patients. Acta Orthop Scand. 1995;66:143–6. - PubMed
-
- Berruti A, Dogliotti L, Bitossi R, Fasolis G, Gorzegno G, Bellina M, Torta M, Porpiglia F, Fontana D, Angeli A. Incidence of skeletal complications in patients with bone metastatic prostate cancer and hormone refractory disease: predictive role of bone resorption and formation markers evaluated at baseline. J Urol. 2000;164:1248–53. - PubMed
-
- Carlin BI, Andriole GL. The natural history, skeletal complications, and management of bone metastases in patients with prostate carcinoma. Cancer. 2000;88:2989–94. - PubMed
-
- Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001;27:165–76. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical