

Comparing cystatin C and creatinine in the diagnosis of pediatric acute renal allograft dysfunction
- PMID: 22207347
- PMCID: PMC3315636
- DOI: 10.1007/s00467-011-2073-9
Comparing cystatin C and creatinine in the diagnosis of pediatric acute renal allograft dysfunction
Abstract
Background: Allograft function following renal transplantation is commonly monitored using serum creatinine. Multiple cross-sectional studies have shown that serum cystatin C is superior to creatinine for detection of mild to moderate chronic kidney dysfunction. Recent data in adults indicate that cystatin C might also be a more sensitive marker of acute renal dysfunction. This study aims to compare cystatin C and creatinine for detection of acute allograft dysfunction in children using pediatric RIFLE (risk of renal dysfunction, injury to the kidney, failure or loss of kidney function, end stage renal disease) criteria for acute kidney injury.
Methods: Retrospective chart review of post-transplant period in 24 patients in whom creatinine and cystatin C were measured every day. Allograft dysfunction was defined as a sustained rise in marker concentration above the mean of the three preceding measurements.
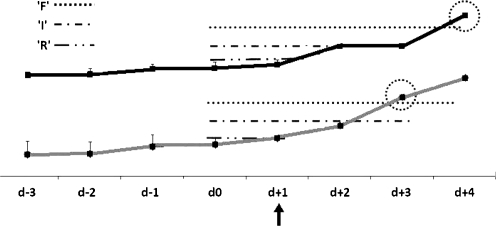
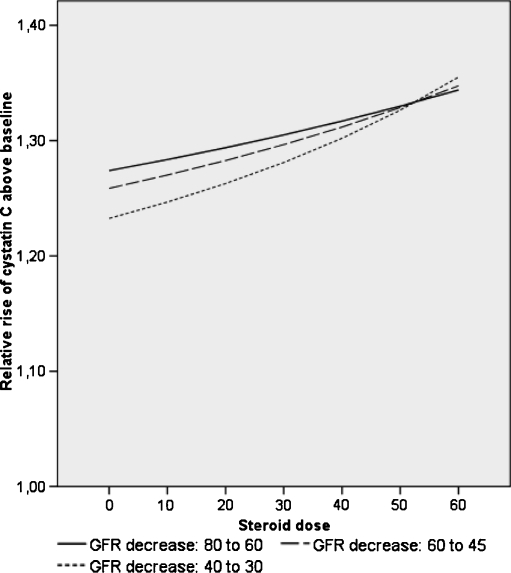
Results: In total, there were 13 episodes of allograft dysfunction. Maximum RIFLE stages with creatinine were 'R' in 7, 'I' in 4, and 'F' in 2, with cystatin C 'R' in 6, 'I' in 4 and 'F' in 3, respectively. In 9/13 cases, both markers rose simultaneously, in three, the rise in creatinine preceded cystatin C by 1-5 days (median 4). In one case, the rise in cystatin C preceded creatinine by 1 day. The time lag was not statistically different. The maximum relative rise of creatinine was significantly higher than cystatin C. By multiple linear regression analysis, the maximum rise of cystatin C was related to the maximum rise of creatinine, but independent of patient age, gender, steroid dose, and anthropometric data.
Conclusions: In this pediatric population, cystatin C was not superior to creatinine for the detection of acute allograft dysfunction.
Figures
References
-
- Perrone RD, Madias NE, Levey AS. Serum creatinine as an index of renal function: new insights into old concepts. Clin Chem. 1992;38:1933–1953. - PubMed
-
- Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am. 1987;34:571–590. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
