

Bone pain and extremely low bone mineral density due to severe vitamin D deficiency in celiac disease
- PMID: 22207878
- PMCID: PMC3235277
- DOI: 10.1007/s11657-011-0059-7
Bone pain and extremely low bone mineral density due to severe vitamin D deficiency in celiac disease
Abstract
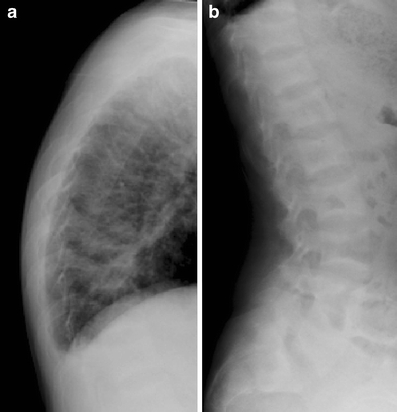
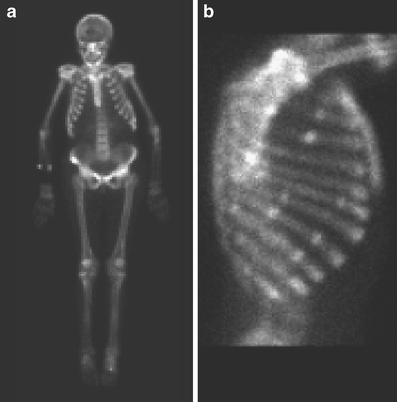
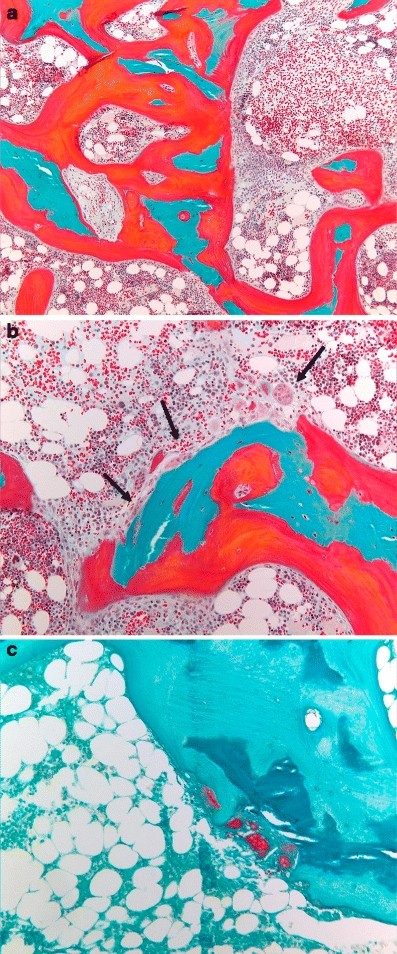
Case report: A 29-year-old wheelchair-bound woman was presented to us by the gastroenterologist with suspected osteomalacia. She had lived in the Netherlands all her life and was born of Moroccan parents. Her medical history revealed iron deficiency, growth retardation, and celiac disease, for which she was put on a gluten-free diet. She had progressive bone pain since 2 years, difficulty with walking, and about 15 kg weight loss. She had a short stature, scoliosis, and pronounced kyphosis of the spine and poor condition of her teeth. Laboratory results showed hypocalcemia, an immeasurable serum 25-hydroxyvitamin D level, and elevated parathyroid hormone and alkaline phosphatase levels. Spinal radiographs showed unsharp, low contrast vertebrae. Bone mineral density measurement at the lumbar spine and hip showed a T-score of -6.0 and -6.5, respectively. A bone scintigraphy showed multiple hotspots in ribs, sternum, mandible, and long bones. A duodenal biopsy revealed villous atrophy (Marsh 3C) and positive antibodies against endomysium, transglutaminase, and gliadin, compatible with active celiac disease. A bone biopsy showed severe osteomalacia but normal bone volume. She was treated with calcium intravenously and later orally. Furthermore, she was treated with high oral doses of vitamin D and a gluten-free diet. After a few weeks of treatment, her bone pain decreased, and her muscle strength improved.
Discussion: In this article, the pathophysiology and occurrence of osteomalacia as a complication of celiac disease are discussed. Low bone mineral density can point to osteomalacia as well as osteoporosis.
Figures
Similar articles
-
Osteomalacia associated with cutaneous psoriasis as the presenting feature of coeliac disease: a case report.Pan Afr Med J. 2012;11:58. Epub 2012 Mar 27. Pan Afr Med J. 2012. PMID: 22593794 Free PMC article.
-
Renal tubular acidosis type 2 with Fanconi's syndrome, osteomalacia, osteoporosis, and secondary hyperaldosteronism in an adult consequent to vitamin D and calcium deficiency: effect of vitamin D and calcium citrate therapy.Endocr Pract. 2006 Sep-Oct;12(5):559-67. doi: 10.4158/EP.12.5.559. Endocr Pract. 2006. PMID: 17002932
-
Osteomalacia caused by atypical renal tubular acidosis with vitamin D deficiency: a case report.CEN Case Rep. 2021 May;10(2):294-300. doi: 10.1007/s13730-020-00561-y. Epub 2021 Jan 4. CEN Case Rep. 2021. PMID: 33398781 Free PMC article.
-
Severe osteomalacia due to gluten-sensitive enteropathy.Ann Ital Med Int. 1994 Jan-Mar;9(1):40-3. Ann Ital Med Int. 1994. PMID: 8003392 Review.
-
Disabling osteomalacic myopathy as the only presenting feature of coeliac disease.Eur J Gastroenterol Hepatol. 2002 Nov;14(11):1271-4. doi: 10.1097/00042737-200211000-00018. Eur J Gastroenterol Hepatol. 2002. PMID: 12439125 Review.
Cited by
-
Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment.Metabolites. 2021 Apr 20;11(4):255. doi: 10.3390/metabo11040255. Metabolites. 2021. PMID: 33924215 Free PMC article. Review.
-
Medication-Related Osteonecrosis of the Jaw (MRONJ): Are Antiresorptive Drugs the Main Culprits or Only Accomplices? The Triggering Role of Vitamin D Deficiency.Nutrients. 2021 Feb 8;13(2):561. doi: 10.3390/nu13020561. Nutrients. 2021. PMID: 33567797 Free PMC article. Review.
-
Bone densitometry in patients with osteomalacia: is it valuable?Clin Cases Miner Bone Metab. 2013 Sep;10(3):180-2. Clin Cases Miner Bone Metab. 2013. PMID: 24554927 Free PMC article. Review.
-
Severe rickets in a young girl caused by celiac disease: the tragedy of delayed diagnosis: a case report.BMC Res Notes. 2014 Oct 8;7:701. doi: 10.1186/1756-0500-7-701. BMC Res Notes. 2014. PMID: 25292220 Free PMC article.
-
Superscan Pattern on Bone Scintigraphy: A Comprehensive Review.Diagnostics (Basel). 2024 Oct 6;14(19):2229. doi: 10.3390/diagnostics14192229. Diagnostics (Basel). 2024. PMID: 39410633 Free PMC article. Review.
References
-
- Balsan S, Garabedian M, Larchet M, Gorski AM, Cournot G, Tau C, Bourdeau A, Silve C, Ricour C. Long-term nocturnal calcium infusions can cure rickets and promote normal mineralization in hereditary resistance to 1,25-dihydroxyvitamin D. J Clin Invest. 1986;77:1661–1667. doi: 10.1172/JCI112483. - DOI - PMC - PubMed
-
- Clements MR, Davies M, Fraser DR, Lumb GA, Mawer EB, Adams PH. Metabolic inactivation of vitamin D is enhanced in primary hyperparathyroidism. Clin Sci Lond. 1987;73:659–664. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
