

Genetic predisposition to peripheral nerve neoplasia: diagnostic criteria and pathogenesis of neurofibromatoses, Carney complex, and related syndromes
- PMID: 22210082
- PMCID: PMC3657472
- DOI: 10.1007/s00401-011-0935-7
Genetic predisposition to peripheral nerve neoplasia: diagnostic criteria and pathogenesis of neurofibromatoses, Carney complex, and related syndromes
Abstract
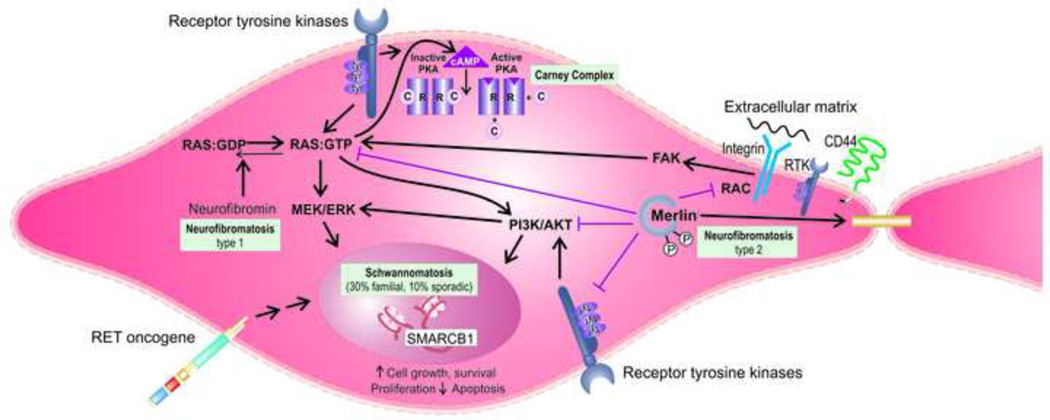
Neoplasms of the peripheral nerve sheath represent essential clinical manifestations of the syndromes known as the neurofibromatoses. Although involvement of multiple organ systems, including skin, central nervous system, and skeleton, may also be conspicuous, peripheral nerve neoplasia is often the most important and frequent cause of morbidity in these patients. Clinical characteristics of neurofibromatosis type 1 (NF1) and neurofibromatosis type 2 (NF2) have been extensively described and studied during the last century, and the identification of mutations in the NF1 and NF2 genes by contemporary molecular techniques have created a separate multidisciplinary field in genetic medicine. In schwannomatosis, the most recent addition to the neurofibromatosis group, peripheral nervous system involvement is the exclusive (or almost exclusive) clinical manifestation. Although the majority of cases of schwannomatosis are sporadic, approximately one-third occur in families and a subset of these has recently been associated with germline mutations in the tumor suppressor gene SMARCB1/INI1. Other curious syndromes that involve the peripheral nervous system are associated with predominant endocrine manifestations, and include Carney complex and MEN2b, secondary to inactivating mutations in the PRKAR1A gene in a subset, and activating mutations in RET, respectively. In this review, we provide a concise update on the diagnostic criteria, pathology and molecular pathogenesis of these enigmatic syndromes in relation to peripheral nerve sheath neoplasia.
Figures
Similar articles
-
Diagnostic Pathology of Tumors of Peripheral Nerve.Neurosurgery. 2021 Feb 16;88(3):443-456. doi: 10.1093/neuros/nyab021. Neurosurgery. 2021. PMID: 33588442 Free PMC article. Review.
-
Germline Mutations for Novel Candidate Predisposition Genes in Sporadic Schwannomatosis.Clin Orthop Relat Res. 2020 Nov;478(11):2442-2450. doi: 10.1097/CORR.0000000000001239. Clin Orthop Relat Res. 2020. PMID: 32281771 Free PMC article.
-
Cancer and Central Nervous System Tumor Surveillance in Pediatric Neurofibromatosis 2 and Related Disorders.Clin Cancer Res. 2017 Jun 15;23(12):e54-e61. doi: 10.1158/1078-0432.CCR-17-0590. Clin Cancer Res. 2017. PMID: 28620005 Review.
-
Neurofibromatosis.Handb Clin Neurol. 2013;111:333-40. doi: 10.1016/B978-0-444-52891-9.00039-7. Handb Clin Neurol. 2013. PMID: 23622184 Review.
-
[Hereditary predisposition to tumors of the central and peripheral nervous systems].Ann Pathol. 2020 Apr;40(2):168-179. doi: 10.1016/j.annpat.2020.02.019. Epub 2020 Mar 17. Ann Pathol. 2020. PMID: 32192808 French.
Cited by
-
Pathology of peripheral nerve sheath tumors: diagnostic overview and update on selected diagnostic problems.Acta Neuropathol. 2012 Mar;123(3):295-319. doi: 10.1007/s00401-012-0954-z. Epub 2012 Feb 12. Acta Neuropathol. 2012. PMID: 22327363 Free PMC article. Review.
-
[Hereditary tumor syndromes in neuropathology].Pathologe. 2017 May;38(3):186-196. doi: 10.1007/s00292-017-0292-y. Pathologe. 2017. PMID: 28474160 Review. German.
-
Malignant melanotic nerve sheath tumor with PRKAR1A, KMT2C, and GNAQ mutations.Free Neuropathol. 2022 Aug 26;3:21. doi: 10.17879/freeneuropathology-2022-3864. eCollection 2022 Jan. Free Neuropathol. 2022. PMID: 37284154 Free PMC article.
-
Multiple Schwannomas of the Spine: Review of the Schwannomatosis or Congenital Neurilemmomatosis: A Case Report.Korean J Spine. 2015 Jun;12(2):91-4. doi: 10.14245/kjs.2015.12.2.91. Epub 2015 Jun 30. Korean J Spine. 2015. PMID: 26217390 Free PMC article.
-
A Case of Malignant Melanotic Schwannoma of the Trigeminal Nerve: A Case Report and Review of Literature.Asian J Neurosurg. 2023 Jun 7;18(2):352-356. doi: 10.1055/s-0043-1768578. eCollection 2023 Jun. Asian J Neurosurg. 2023. PMID: 37397058 Free PMC article.
References
-
- National Institutes of Health Consensus Development Conference Statement: Neurofibromatosis. Arch Neurol. 1988;45:575–578. - PubMed
-
- Consensus Development Panel. National Institutes of Health Consensus Development Conference Statement n Acoustic Neuroma. Arch Neurol. 1994;51:201–207. - PubMed
-
- Almeida MQ, Muchow M, Boikos S, Bauer AJ, Griffin KJ, Tsang KM, Cheadle C, Watkins T, Wen F, Starost MF, Bossis I, Nesterova M, Stratakis CA. Mouse Prkar1a haploinsufficiency leads to an increase in tumors in the Trp53+/− or Rb1+/− backgrounds and chemically induced skin papillomas by dysregulation of the cell cycle and Wnt signaling. Hum Mol Genet. 2010;19:1387–1398. - PMC - PubMed
-
- Amieux PS, Cummings DE, Motamed K, Brandon EP, Wailes LA, Le K, Idzerda RL, McKnight GS. Compensatory regulation of RIalpha protein levels in protein kinase A mutant mice. J Biol Chem. 1997;272:3993–3998. - PubMed
-
- Antinheimo J, Sankila R, Carpen O, Pukkala E, Sainio M, Jaaskelainen J. Population-based analysis of sporadic and type 2 neurofibromatosis-associated meningiomas and schwannomas. Neurology. 2000;54:71–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
