

Characterization of macular lesions in punctate inner choroidopathy with spectral domain optical coherence tomography
- PMID: 22210152
- PMCID: PMC3438299
- DOI: 10.1007/s12348-011-0054-6
Characterization of macular lesions in punctate inner choroidopathy with spectral domain optical coherence tomography
Abstract
Purpose: Punctate inner choroidopathy (PIC) is an ocular inflammatory disease. Spectral domain optical coherence tomography (SD-OCT) allows detailed visualization of retinal and choroidal structures. We aimed to describe the retinal changes on SD-OCT associated with PIC lesions localized in the macula.
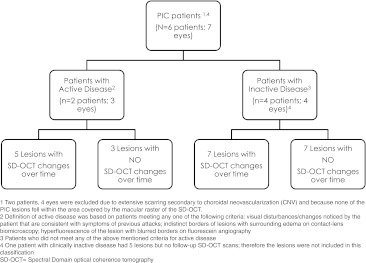
Methods: Retrospective case series: PIC lesions not associated with choroidal neovascularization (CNV) and captured by macular SD-OCT scans were identified and characterized.
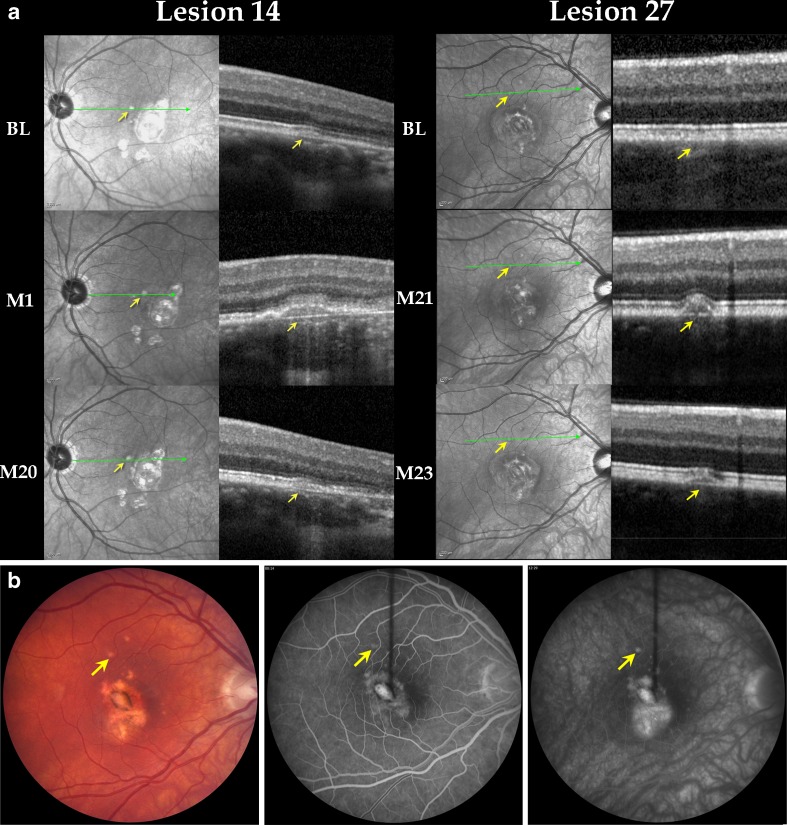
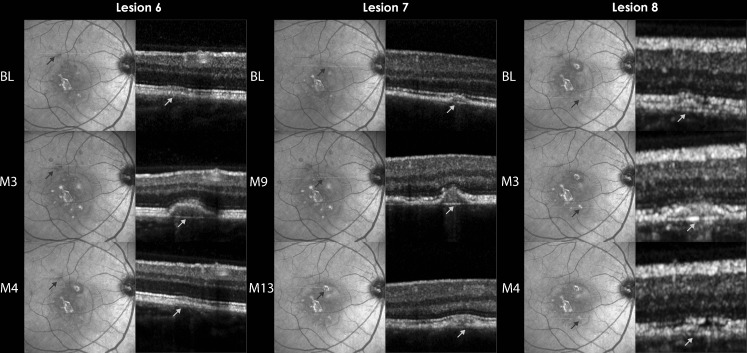
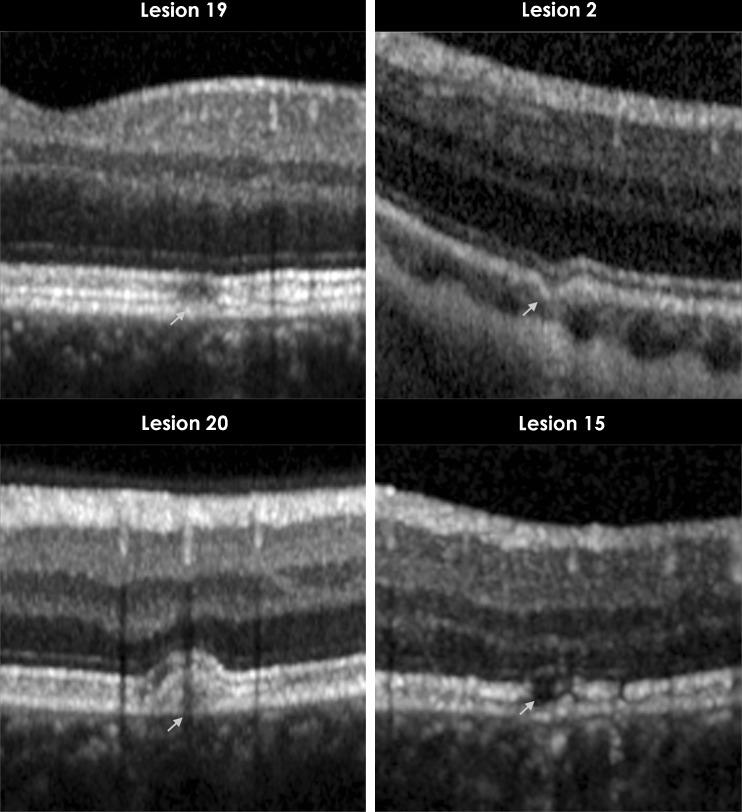
Results: Twenty-seven PIC lesions from seven patients (eight eyes) were identified and classified into four categories according to disease activity and temporal changes. Among clinically inactive patients, two main patterns were noted on OCT: (1) retinal pigment epithelium (RPE) elevation with sub-RPE hyper-reflective signals and (2) localized disruption of outer retinal layers with choroid and Bruch's membrane (BM) generally spared. Clinically active patients demonstrated lesions with intact BM with RPE elevation that fluctuated with disease activity and sub-RPE hyper-reflective signals. Photoreceptor-associated bands on SD-OCT (PRs) were not visible during active disease, but returned to normal visibility when lesions were clinically stable. Seven lesions in patients without clinically detected activity demonstrated alteration of RPE elevation.
Conclusion: SD-OCT can provide detailed structural characteristics of PIC lesions. RPE elevation is noted in many lesions while BM and choroid are spared. Photoreceptor-associated bands on SD-OCT appear compressed during clinically active stages and are visible during stabilization. OCT may provide information on activity not detected clinically.
Figures
References
LinkOut - more resources
Full Text Sources
