

Nonalcoholic fatty liver disease is associated with left ventricular diastolic dysfunction in patients with type 2 diabetes
- PMID: 22210573
- PMCID: PMC3263884
- DOI: 10.2337/dc11-1820
Nonalcoholic fatty liver disease is associated with left ventricular diastolic dysfunction in patients with type 2 diabetes
Abstract
Objective: Data on cardiac function in patients with nonalcoholic fatty liver disease (NAFLD) are limited and conflicting. We assessed whether NAFLD is associated with abnormalities in cardiac function in patients with type 2 diabetes.
Research design and methods: We studied 50 consecutive type 2 diabetic individuals without a history of ischemic heart disease, hepatic diseases, or excessive alcohol consumption, in whom NAFLD was diagnosed by ultrasonography. A tissue Doppler echocardiography with myocardial strain measurement was performed in all patients.
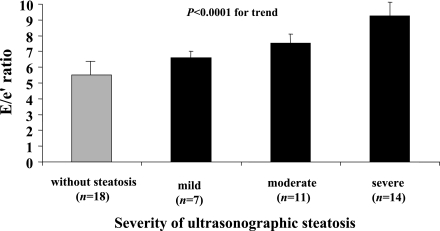
Results: Thirty-two patients (64%) had NAFLD, and when compared with the other 18 patients, age, sex, BMI, waist circumference, hypertension, smoking, diabetes duration, microvascular complication status, and medication use were not significantly different. In addition, the left ventricular (LV) mass and volumes, ejection fraction, systemic vascular resistance, arterial elasticity, and compliance were also not different. NAFLD patients had lower e' (8.2 ± 1.5 vs. 9.9 ± 1.9 cm/s, P < 0.005) tissue velocity, higher E-to-e' ratio (7.90 ± 1.3 vs. 5.59 ± 1.1, P < 0.0001), a higher time constant of isovolumic relaxation (43.1 ± 10.1 vs. 33.2 ± 12.9 ms, P < 0.01), higher LV-end diastolic pressure (EDP) (16.5 ± 1.1 vs. 15.1 ± 1.0 mmHg, P < 0.0001), and higher LV EDP/end diastolic volume (0.20 ± 0.03 vs. 0.18 ± 0.02 mmHg, P < 0.05) than those without steatosis. Among the measurements of LV global longitudinal strain and strain rate, those with NAFLD also had higher E/global longitudinal diastolic strain rate during the early phase of diastole (E/SR(E)). All of these differences remained significant after adjustment for hypertension and other cardiometabolic risk factors.
Conclusions: Our data show that in patients with type 2 diabetes and NAFLD, even if the LV morphology and systolic function are preserved, early features of LV diastolic dysfunction may be detected.
Figures
References
-
- Finucane MM, Stevens GA, Cowan MJ, et al. ; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Body Mass Index) National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet 2011;377:557–567 - PMC - PubMed
-
- Fang ZY, Prins JB, Marwick TH. Diabetic cardiomyopathy: evidence, mechanisms, and therapeutic implications. Endocr Rev 2004;25:543–567 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
