

Cardiopulmonary function in individuals with HIV infection in the antiretroviral therapy era
- PMID: 22210636
- PMCID: PMC3606053
- DOI: 10.1097/QAD.0b013e32835099ae
Cardiopulmonary function in individuals with HIV infection in the antiretroviral therapy era
Abstract
Objective: To determine relationship of echocardiographic measures of pulmonary hypertension to lung function and inflammatory biomarkers in HIV-infected individuals.
Design: Cross-sectional study of 116 HIV-infected outpatients.
Methods: Doppler-echocardiography and pulmonary function testing were performed. Induced sputum and plasma cytokines, sputum cell counts and differentials, markers of peripheral T-cell activation, and serum N-terminal pro-brain natriuretic peptide (NT-proBNP) were measured. Univariate and multivariate analyses determined relationship of echocardiographic variables to pulmonary function, inflammation, and NT-proBNP.
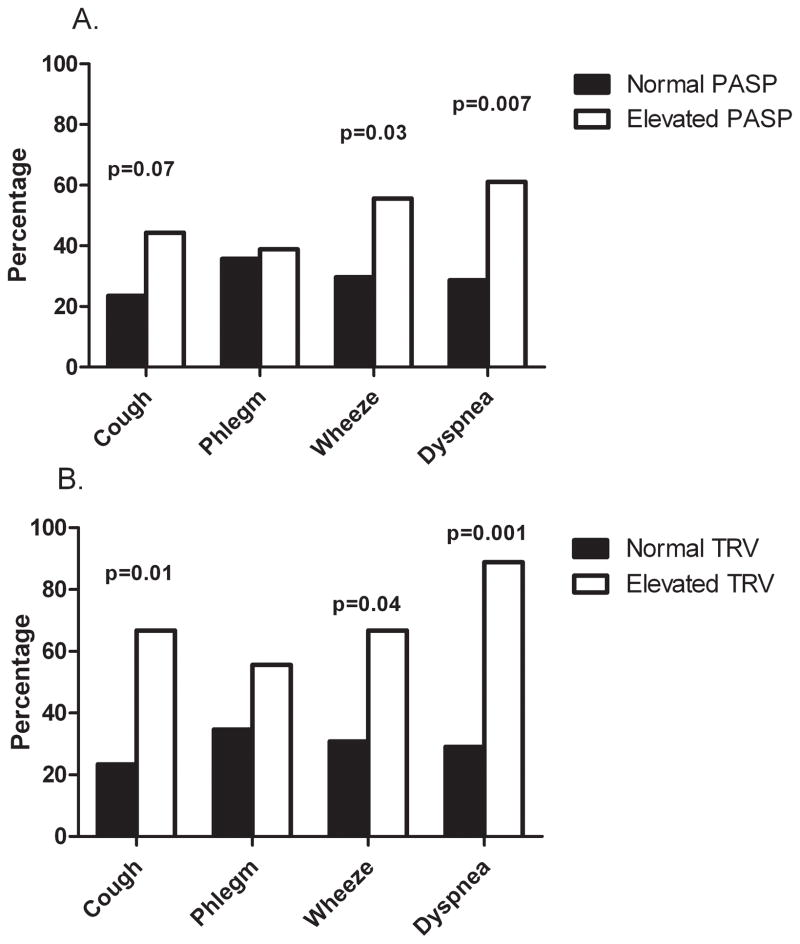
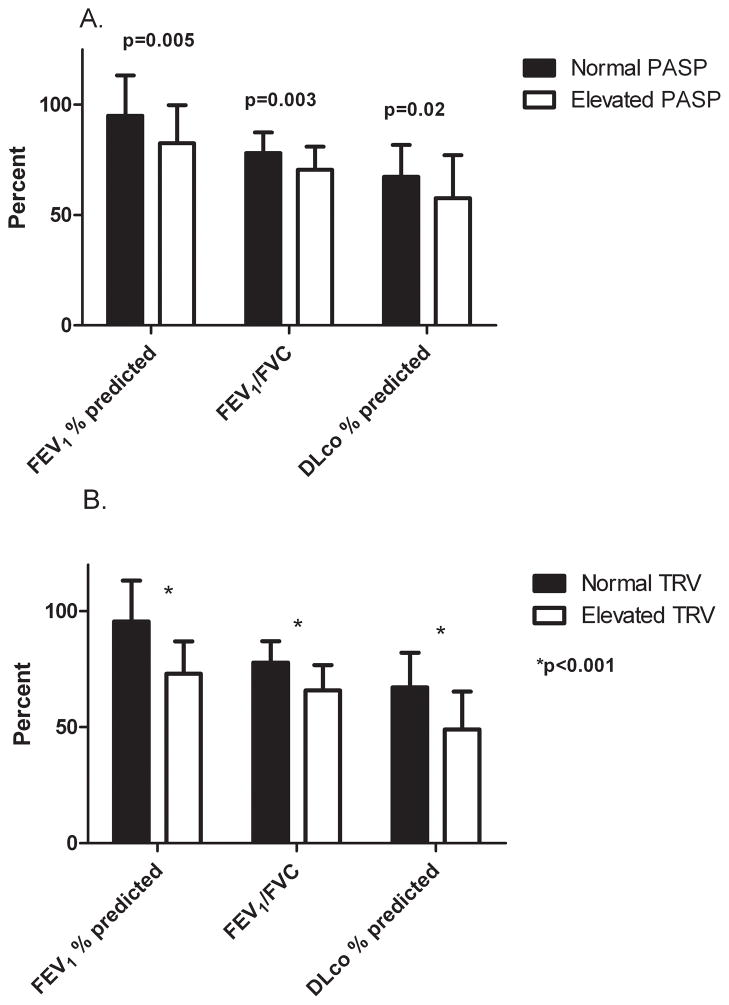
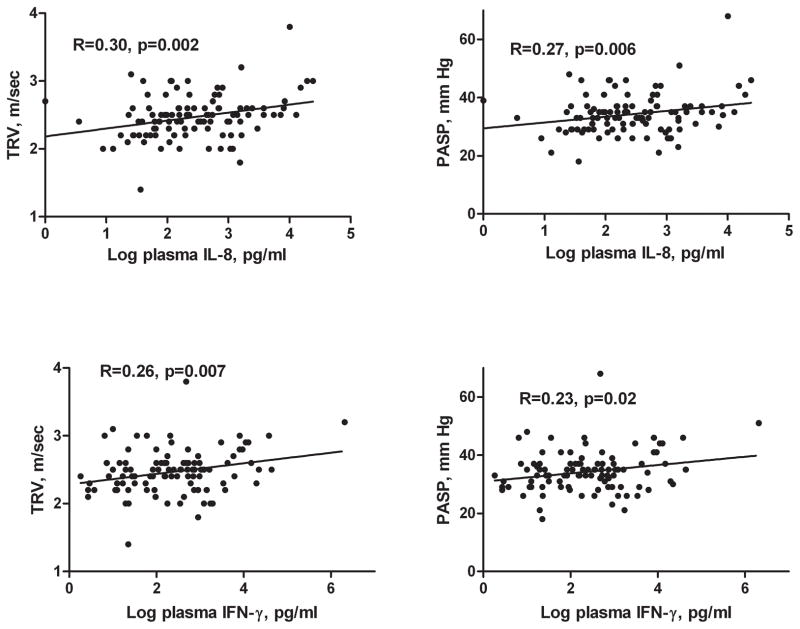
Results: Mean estimated pulmonary artery systolic pressure (PASP) was 34.3 mmHg (SD 6.9) and mean tricuspid regurgitant jet velocity (TRV) was 2.5 m/s (SD 0.32). Eighteen participants (15.5%) had PASP of at least 40 mmHg, and nine (7.8%) had TRV of at least 3.0 m/s. Elevated TRV was significantly associated with CD4 cell counts below 200 cells/μl and higher log HIV-RNA levels. Forced expiratory volume in 1 s (FEV(1)) percentage predicted, FEV(1)/forced vital capacity, and diffusing capacity for carbon monoxide (DLco) percentage predicted were significantly lower in those with elevated PASP or TRV. Sputum interleukin-8, peripheral interleukin-8, peripheral interferon-γ levels, and CD8(+) T-cell expression of CD69(+) were associated with increasing PASP and TRV. Log NT-proBNP was significantly higher with increasing PASP and TRV. Left ventricular function was not associated with PASP or TRV.
Conclusion: Echocardiographic manifestations of pulmonary hypertension are common in HIV and are associated with respiratory symptoms, more advanced HIV disease, airway obstruction, abnormal DLco, and systemic and pulmonary inflammation. Pulmonary hypertension and chronic obstructive pulmonary disease coexist in HIV and may arise secondary to common inflammatory mechanisms.
Conflict of interest statement
Conflicts of interest: For the remaining authors, none were declared.
Figures
References
-
- Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532–555. - PubMed
-
- Crothers K, Butt AA, Gibert CL, Rodriguez-Barradas MC, Crystal S, Justice AC. Increased COPD among HIV-positive compared to HIV-negative veterans. Chest. 2006;130:1326–1333. - PubMed
-
- Diaz PT, King MA, Pacht ER, Wewers MD, Gadek JE, Nagaraja HN, et al. Increased susceptibility to pulmonary emphysema among HIV-seropositive smokers. Ann Intern Med. 2000;132:369–372. - PubMed
-
- Speich R, Jenni R, Opravil M, Pfab M, Russi EW. Primary pulmonary hypertension in HIV infection. Chest. 1991;100:1268–1271. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
