

How I treat childhood CML
- PMID: 22210880
- PMCID: PMC3293638
- DOI: 10.1182/blood-2011-10-380774
How I treat childhood CML
Abstract
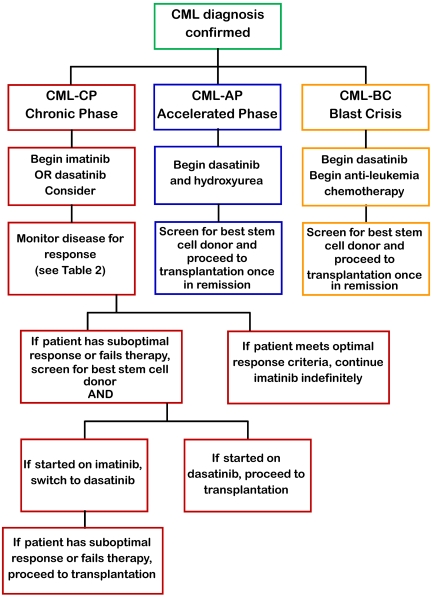
Chronic myeloid leukemia (CML) is composed of 3% of pediatric leukemias, making evidence-based recommendations difficult. Imatinib has revolutionized the treatment for adult CML by eliminating allogeneic stem cell transplantation for almost all patients in chronic phase. Shown effective in pediatric CML, imatinib and successive tyrosine kinase inhibitors (TKI) have provided more therapeutic options. Because stem cell transplantation has been better tolerated in children and adolescents, the decision to treat by either TKI or transplantation is controversial. We present a recent case of a 12-month-old boy diagnosed with BCR-ABL(+) CML to highlight the controversies in treatment recommendations. We review the pediatric stem cell transplantation outcomes as well as the pediatric experience with imatinib and other TKIs. Finally, we compare the side effects as well as costs associated with allogeneic stem cell transplantation versus TKI therapy. We recommend that frontline therapy for pediatric CML in chronic phase is TKI therapy without transplantation. Patients in accelerated or blast crisis or who fail to reach landmarks on TKIs either because of intolerance or resistance should pursue stem cell transplantation. Although we recommend adopting adult clinical experience to guide therapeutic decision making, the issues of infant CML, drug formulation, pharmacokinetics, and adolescent compliance merit clinical investigation.
Figures
Similar articles
-
Chronic myelogenous leukemia.Clin J Oncol Nurs. 2005 Oct;9(5):535-8. doi: 10.1188/05.CJON.535-538. Clin J Oncol Nurs. 2005. PMID: 16235580 Review.
-
Successful treatment of lymphoid blastic crisis in chronic myelogenous leukemia with the additional bcr/abl transcript using imatinib-combined chemotherapy and high-dose chemotherapy with allogeneic bone marrow stem cell transplantation.Int J Hematol. 2011 Dec;94(6):561-6. doi: 10.1007/s12185-011-0956-y. Epub 2011 Nov 8. Int J Hematol. 2011. PMID: 22057509
-
Double minutes containing amplified bcr-abl fusion gene in a case of chronic myeloid leukemia treated by imatinib.Eur J Haematol. 2003 Apr;70(4):235-9. doi: 10.1034/j.1600-0609.2003.00046.x. Eur J Haematol. 2003. PMID: 12656747
-
[Current therapy concepts in chronic myeloid leukemia. Study IV of the German CML Study Group].Internist (Berl). 2002 Oct;43(10):1228, 1231-8, 1241-4. doi: 10.1007/s00108-002-0706-6. Internist (Berl). 2002. PMID: 12524904 Review. German. No abstract available.
-
Imatinib (ST1571) provides only limited selectivity for CML cells and treatment might be complicated by silent BCR-ABL genes.Cancer Biol Ther. 2003 Jan-Feb;2(1):103-8. doi: 10.4161/cbt.240. Cancer Biol Ther. 2003. PMID: 12673129
Cited by
-
The role of stem cell transplantation for chronic myelogenous leukemia in the 21st century.Blood. 2015 May 21;125(21):3230-5. doi: 10.1182/blood-2014-10-567784. Epub 2015 Apr 7. Blood. 2015. PMID: 25852053 Free PMC article. Review.
-
Efficacy of imatinib mesylate-based front-line therapy in pediatric chronic myelogenous leukemia.Korean J Pediatr. 2013 Aug;56(8):343-50. doi: 10.3345/kjp.2013.56.8.343. Epub 2013 Aug 27. Korean J Pediatr. 2013. PMID: 24019845 Free PMC article.
-
Chronic Myeloid Leukemia in India.J Glob Oncol. 2016 Jul 20;3(1):64-71. doi: 10.1200/JGO.2015.002667. eCollection 2017 Feb. J Glob Oncol. 2016. PMID: 28717743 Free PMC article. Review.
-
Long-term safety and efficacy of imatinib in pediatric patients with chronic myeloid leukemia: single-center experience from China.Int J Hematol. 2021 Mar;113(3):413-421. doi: 10.1007/s12185-020-03042-1. Epub 2021 Jan 1. Int J Hematol. 2021. PMID: 33386594
-
Paediatric chronic myeloid leukaemia: Is it really a different disease?Indian J Med Res. 2019 May;149(5):600-609. doi: 10.4103/ijmr.IJMR_331_19. Indian J Med Res. 2019. PMID: 31417027 Free PMC article. Review.
References
-
- Petridou ET, Sergentanis TN, Panagopoulou P, et al. In vitro fertilization and risk of childhood leukemia in Greece and Sweden. [published online ahead of print, May 25, 2011]. Pediar Blood Cancer. doi: 10.1002/pbc.23194. - DOI - PubMed
-
- Ries LAG SM, Gurney JG, Linet M, Tamra T, Young JL, Bunin GR, editors. Bethesda, MD: National Cancer Institute, SEER Program; 1999. Cancer Incidence and Survival Among Children and Adolescents: United States SEER Program 1975-1995 (NIH publication no. 99-4649).
-
- Homans AC, Young PC, Dickerman JD, Land ML. Adult-type CML in childhood: case report and review. Am J Pediatr Hematol Oncol. 1984;6(2):220–224. - PubMed
-
- Castro-Malaspina H, Schaison G, Briere J, et al. Philadelphia chromosome-positive chronic myelocytic leukemia in children: survival and prognostic factors. Cancer. 1983;52(4):721–727. - PubMed
-
- Millot F, Traore P, Guilhot J, et al. Clinical and biological features at diagnosis in 40 children with chronic myeloid leukemia. Pediatrics. 2005;116(1):140–143. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
