

Pathophysiology of hypercortisolism in depression: pituitary and adrenal responses to low glucocorticoid feedback
- PMID: 22211368
- PMCID: PMC3893569
- DOI: 10.1111/j.1600-0447.2011.01821.x
Pathophysiology of hypercortisolism in depression: pituitary and adrenal responses to low glucocorticoid feedback
Abstract
Objective: To test three theories of hypercortisolemia in depression-hypothalamic overdrive, impaired glucocorticoid feedback, or autonomous cortisol production.
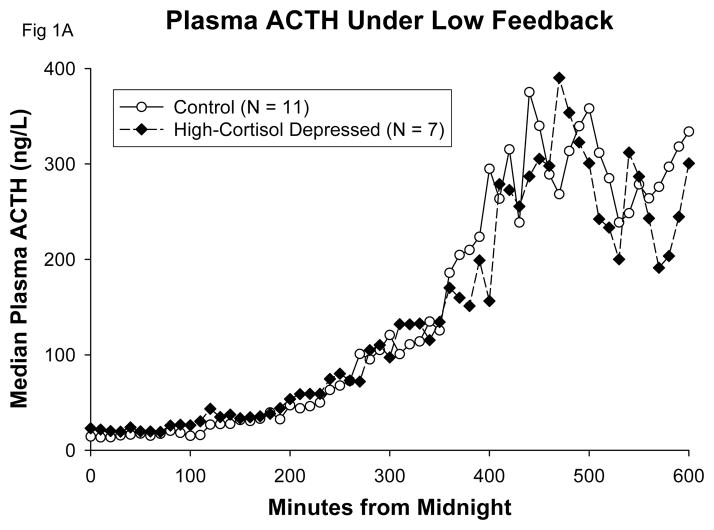
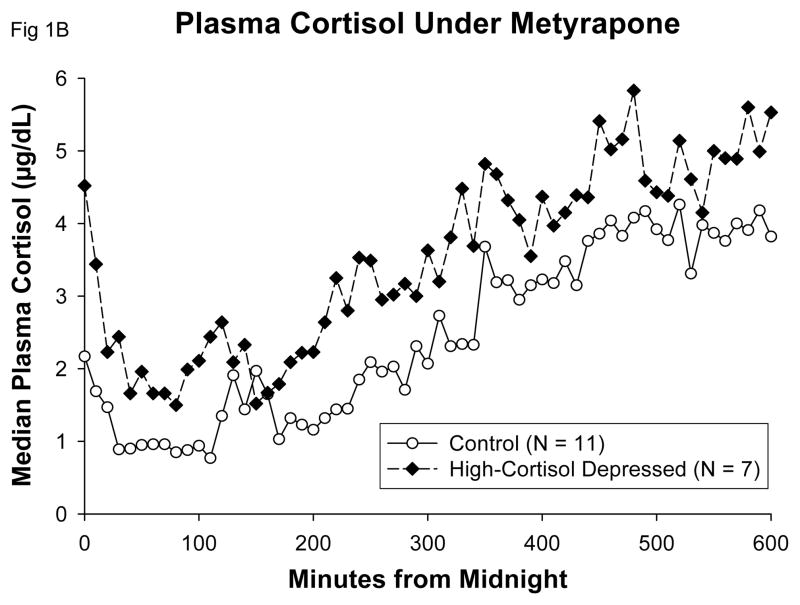
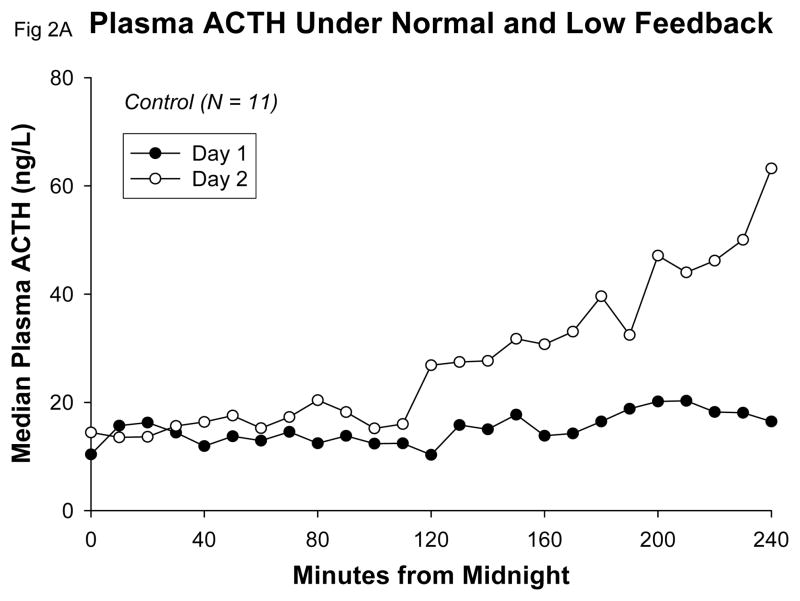
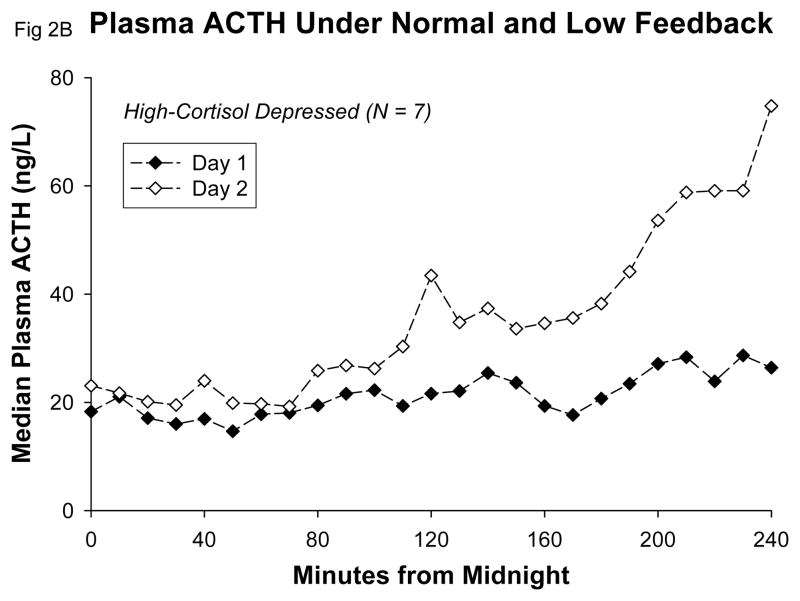
Method: We applied an overnight low-cortisol feedback strategy by administering metyrapone to hypercortisolemic depressed in-patients and control subjects.
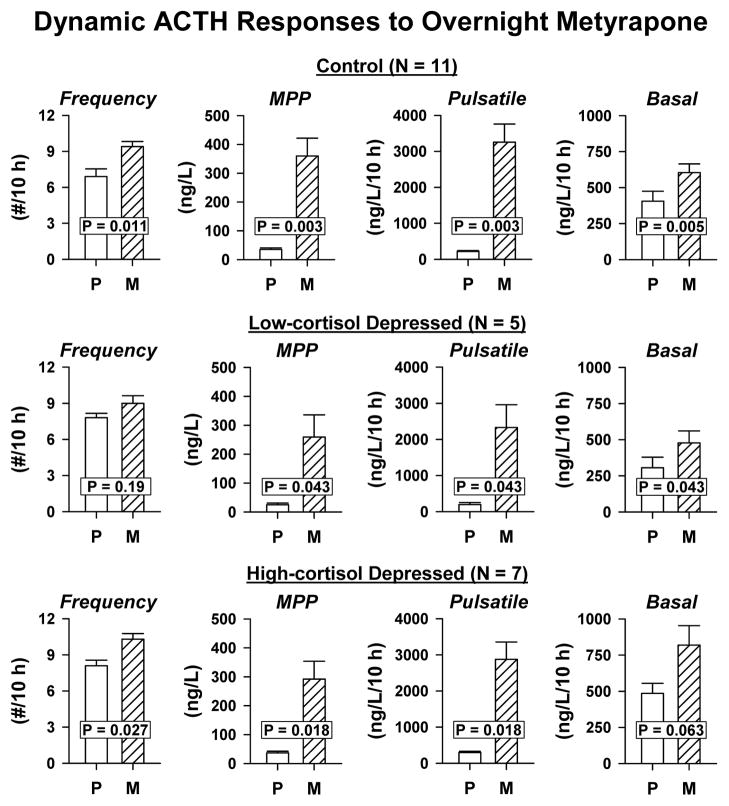
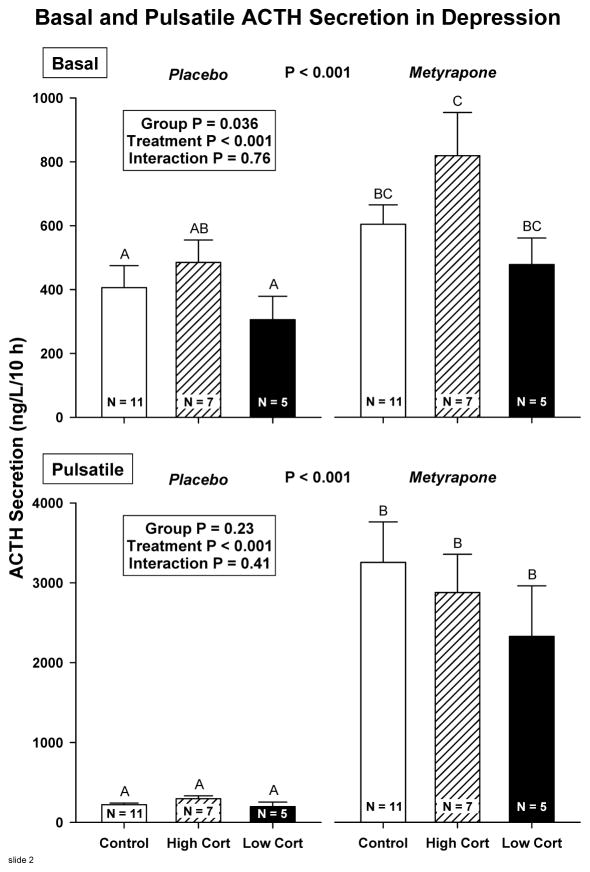
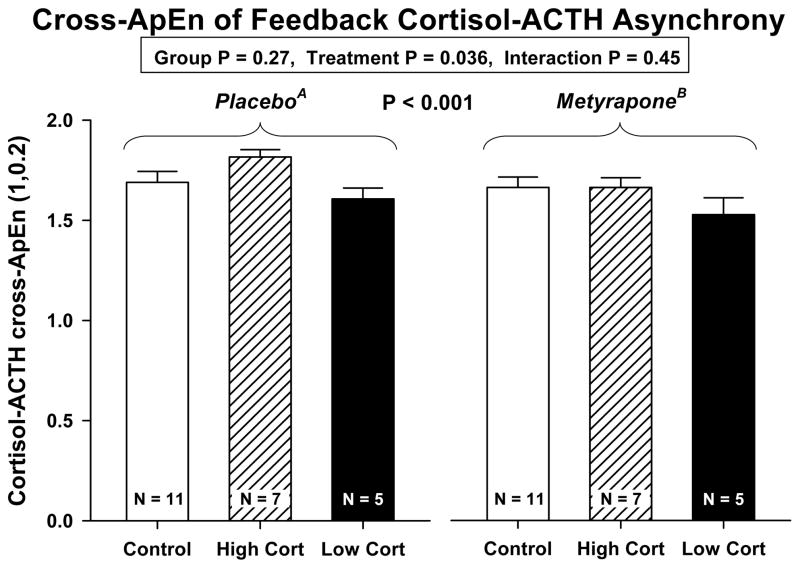
Results: Under metyrapone, the increases of plasma adrenocorticotropic hormone (ACTH) concentrations and of basal and pulsatile ACTH secretion were not exaggerated in hypercortisolemic depressed patients compared with control subjects. ACTH approximate entropy (ApEn) did not differ at baseline or under metyrapone. Thus, neither hypothalamic overdrive nor irregular ACTH secretion was seen. We did not detect impaired cortisol feedback: the ACTH response was not reduced, and ApEn measures that are sensitive to feedback changes were comparable in both groups. Metyrapone disrupted cortisol secretory regularity in depressed and control subjects. On the baseline day, basal cortisol secretion was significantly increased and was highly irregular (high ApEn), and ACTH-cortisol cross-ApEn was markedly elevated in high-cortisol patients.
Conclusion: Classical feed-forward overdrive and impaired feedback theories of hypercortisolemia in depression were not supported. Depressive hypercortisolemia may result from alternative pathophysiological mechanisms involving irregular basal hypersecretion of cortisol, associated with adrenal enlargement, possibly through splanchnic sympathetic activation of the adrenal cortex.
© 2011 John Wiley & Sons A/S.
Conflict of interest statement
No part of this work has been previously published or is under consideration for publication elsewhere. The authors have no competing financial interests in relation to this work. In the past 3 years, Dr. Bernard Carroll has received compensation from AstraZeneca, MultiHealth Systems (licensee for the Carroll Depression Scales), South Carolina Psychiatric Association, Springer Publishing Company and Brentwood Biomedical Research Institute, Los Angeles. Dr. Frederick Cassidy has had a grant from Pfizer.
Figures
References
-
- RUBIN RT, MANDELL AJ. Adrenal cortical activity in pathological emotional states: a review. Am J Psychiatry. 1966;123(4):387–400. - PubMed
-
- SACHAR EJ, HELLMAN L, FUKUSHIMA DK, GALLAGHER TF. Cortisol production in depressive illness. A clinical and biochemical clarification. Arch Gen Psychiatry. 1970;23(4):289–298. - PubMed
-
- NEMEROFF CB, WIDERLOV E, BISSETTE G, et al. Elevated concentrations of CSF corticotropin-releasing factor-like immunoreactivity in depressed patients. Science. 1984;226(4680):1342–1344. - PubMed
-
- UR E, DINAN TG, O’KEANE V, et al. Effect of metyrapone on the pituitary-adrenal axis in depression: relation to dexamethasone suppressor status. Neuroendocrinol. 1992;56(4):533–538. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
