

Obesity, leptin, and Alzheimer's disease
- PMID: 22211890
- PMCID: PMC3564488
- DOI: 10.1111/j.1749-6632.2011.06274.x
Obesity, leptin, and Alzheimer's disease
Abstract
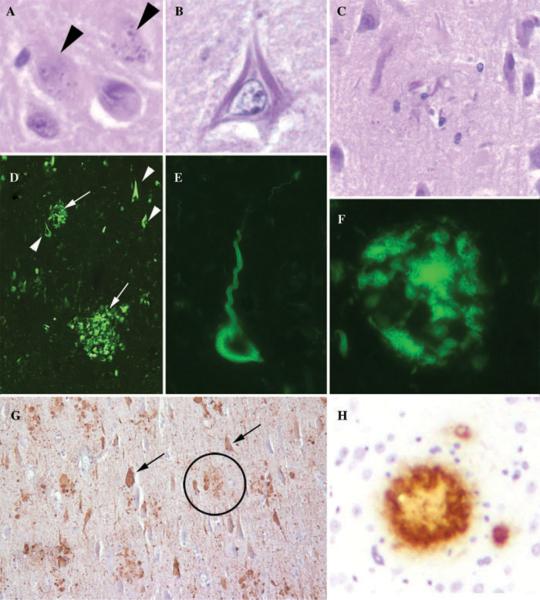
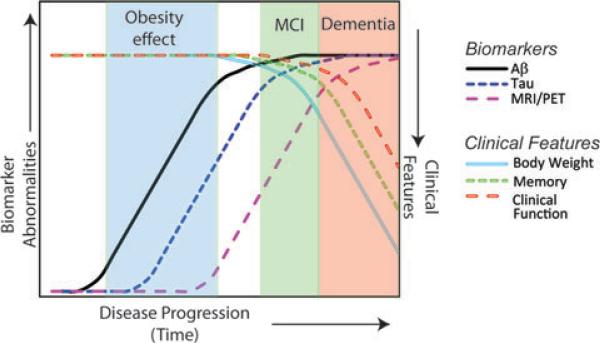
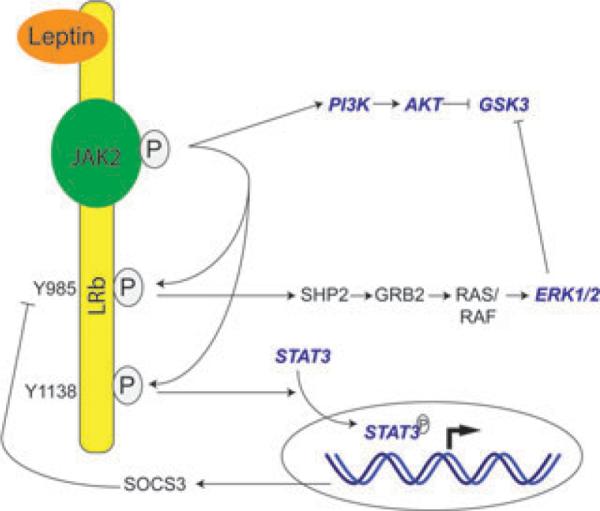
Obesity has various deleterious effects on health largely associated with metabolic abnormalities including abnormal glucose and lipid homeostasis that are associated with vascular injury and known cardiac, renal, and cerebrovascular complications. Advanced age is also associated with increased adiposity, decreased lean mass, and increased risk for obesity-related diseases. Although many of these obesity- and age-related disease processes have long been subsumed to be secondary to metabolic or vascular dysfunction, increasing evidence indicates that obesity also modulates nonvascular diseases such as Alzheimer's disease (AD) dementia. The link between peripheral obesity and neurodegeneration will be explored, using adipokines and AD as a template. After an introduction to the neuropathology of AD, the relationship between body weight, obesity, and dementia will be reviewed. Then, population-based and experimental studies that address whether leptin modulates brain health and mitigates AD pathways will be explored. These studies will serve as a framework for understanding the role of adipokines in brain health.
© 2011 New York Academy of Sciences.
Figures
References
-
- Whitmer RA. The epidemiology of adiposity and dementia. Curr. Alzheimer Res. 2007;4:117–122. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
