

Comparison of hospital risk-standardized mortality rates calculated by using in-hospital and 30-day models: an observational study with implications for hospital profiling
- PMID: 22213491
- PMCID: PMC3319769
- DOI: 10.7326/0003-4819-156-1-201201030-00004
Comparison of hospital risk-standardized mortality rates calculated by using in-hospital and 30-day models: an observational study with implications for hospital profiling
Erratum in
- Ann Intern Med. 2012 Mar 6;156(5):404
Abstract
Background: In-hospital mortality measures, which are widely used to assess hospital quality, are not based on a standardized follow-up period and may systematically favor hospitals with shorter lengths of stay (LOSs).
Objective: To assess the agreement between performance measures of U.S. hospitals by using risk-standardized in-hospital and 30-day mortality rates.
Design: Observational study.
Setting: Nonfederal acute care hospitals in the United States with at least 30 admissions for acute myocardial infarction (AMI), heart failure (HF), and pneumonia from 2004 to 2006.
Patients: Medicare fee-for-service patients admitted for AMI, HF, or pneumonia from 2004 to 2006.
Measurements: The primary outcomes were in-hospital and 30-day risk-standardized mortality rates (RSMRs).
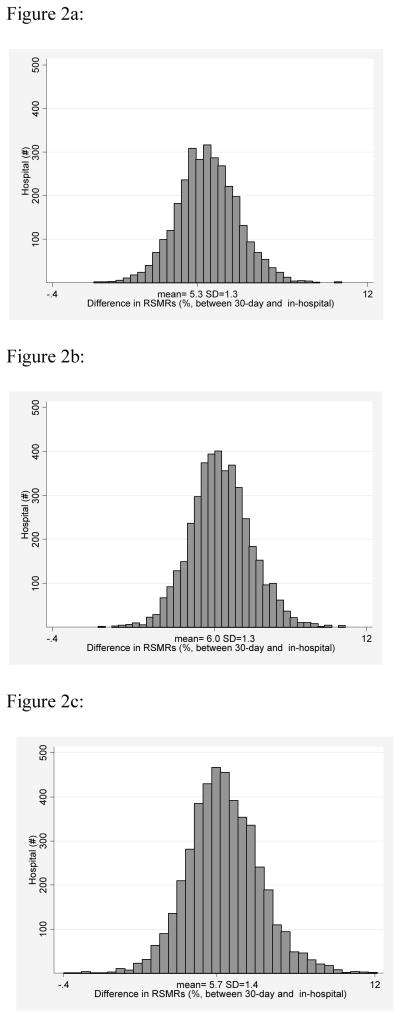
Results: Included patients comprised 718,508 admissions to 3135 hospitals for AMI, 1,315,845 admissions to 4209 hospitals for HF, and 1,415,237 admissions to 4498 hospitals for pneumonia. The hospital-level mean patient LOS varied across hospitals for each condition, ranging from 2.3 to 13.7 days for AMI, 3.5 to 11.9 days for HF, and 3.8 to 14.8 days for pneumonia. The mean RSMR differences (30-day RSMR minus in-hospital RSMR) were 5.3% (SD, 1.3) for AMI, 6.0% (SD, 1.3) for HF, and 5.7% (SD, 1.4) for pneumonia; distributions varied widely across hospitals. Performance classifications differed between the in-hospital and 30-day models for 257 hospitals (8.2%) for AMI, 456 (10.8%) for HF, and 662 (14.7%) for pneumonia. Hospital mean LOS was positively correlated with in-hospital RSMRs for all 3 conditions.
Limitation: Medicare claims data were used for risk adjustment.
Conclusion: In-hospital mortality measures provide a different assessment of hospital performance than 30-day mortality and are biased in favor of hospitals with shorter LOSs.
Primary funding source: The Centers for Medicare & Medicaid Services and National Heart, Lung, and Blood Institute.
Figures

References
-
- Piantadosi S. Clinical trials: a methodologic perspective. New York: John Wiley and Sons, Inc; 1997.
-
- Agency for Healthcare Research and Quality. Inpatient Quality Indicators Overview - AHRQ Quality Indicators. 2006.
-
- Agency for Healthcare Research and Quality. Health Care Report Card Compendium. - PubMed
-
- Baker DW, Einstadter D, Thomas CL, Husak SS, Gordon NH, Cebul RD. Mortality trends during a program that publicly reported hospital performance. Medical care. 2002;40(10):879–90. - PubMed
-
- Jencks SF, Williams DK, Kay TL. Assessing hospital-associated deaths from discharge data. The role of length of stay and comorbidities. JAMA. 1988;260(15):2240–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous