

Cost-effectiveness of long-term outpatient buprenorphine-naloxone treatment for opioid dependence in primary care
- PMID: 22215271
- PMCID: PMC3358393
- DOI: 10.1007/s11606-011-1962-8
Cost-effectiveness of long-term outpatient buprenorphine-naloxone treatment for opioid dependence in primary care
Abstract
Background: Primary care physicians with appropriate training may prescribe buprenorphine-naloxone (bup/nx) to treat opioid dependence in US office-based settings, where many patients prefer to be treated. Bup/nx is off patent but not available as a generic.
Objective: We evaluated the cost-effectiveness of long-term office-based bup/nx treatment for clinically stable opioid-dependent patients compared to no treatment.
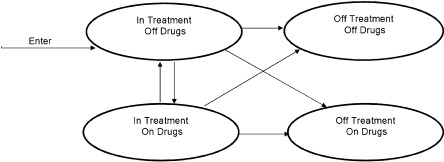
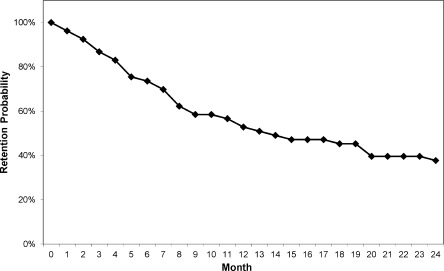
Design, subjects, and intervention: A decision analytic model simulated a hypothetical cohort of clinically stable opioid-dependent individuals who have already completed 6 months of office-based bup/nx treatment. Data were from a published cohort study that collected treatment retention, opioid use, and costs for this population, and published quality-of-life weights. Uncertainties in estimated monthly costs and quality-of-life weights were evaluated in probabilistic sensitivity analyses, and the economic value of additional research to reduce these uncertainties was also evaluated.
Main measures: Bup/nx, provider, and patient costs in 2010 US dollars, quality-adjusted life years (QALYs), and incremental cost-effectiveness (CE) ratios ($/QALY); costs and QALYs are discounted at 3% annually.
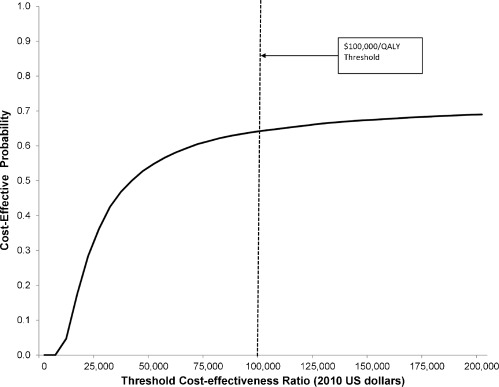
Key results: In the base case, office-based bup/nx for clinically stable patients has a CE ratio of $35,100/QALY compared to no treatment after 24 months, with 64% probability of being < $100,000/QALY in probabilistic sensitivity analysis. With a 50% bup/nx price reduction the CE ratio is $23,000/QALY with 69% probability of being < $100,000/QALY. Alternative quality-of-life weights result in CE ratios of $138,000/QALY and $90,600/QALY. The value of research to reduce quality-of-life uncertainties for 24-month results is $6,400 per person eligible for treatment at the current bup/nx price and $5,100 per person with a 50% bup/nx price reduction.
Conclusions: Office-based bup/nx for clinically stable patients may be a cost-effective alternative to no treatment at a threshold of $100,000/QALY depending on assumptions about quality-of-life weights. Additional research about quality-of-life benefits and broader health system and societal cost savings of bup/nx therapy is needed.
Trial registration: ClinicalTrials.gov NCT00078130.
Figures
References
-
- Results from the 2009 National Survey on Drug Use and Health: Volume 1. Summary of National Findings. http://oas.samhsa.gov/NSDUH/2k9NSDUH/2k9Results.htm. Accessed November 10, 2011.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
