

Transcriptionally active syncytial aggregates in the maternal circulation may contribute to circulating soluble fms-like tyrosine kinase 1 in preeclampsia
- PMID: 22215706
- PMCID: PMC3319764
- DOI: 10.1161/HYPERTENSIONAHA.111.182170
Transcriptionally active syncytial aggregates in the maternal circulation may contribute to circulating soluble fms-like tyrosine kinase 1 in preeclampsia
Abstract
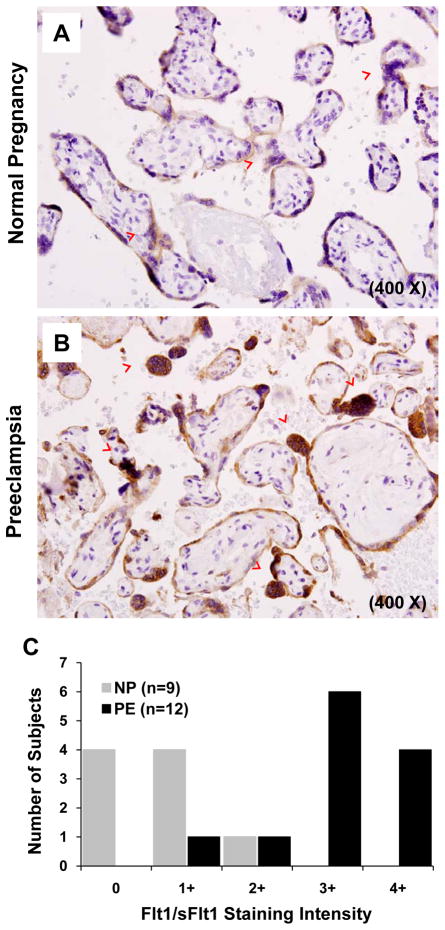
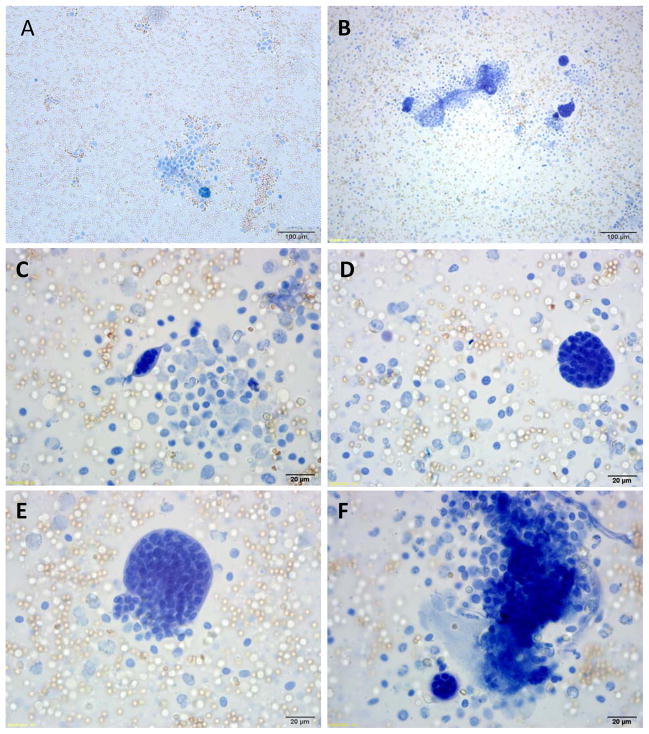
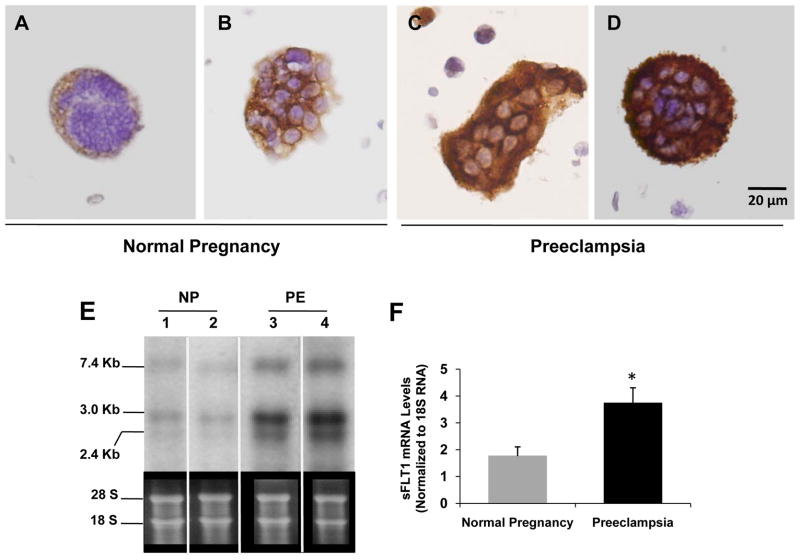
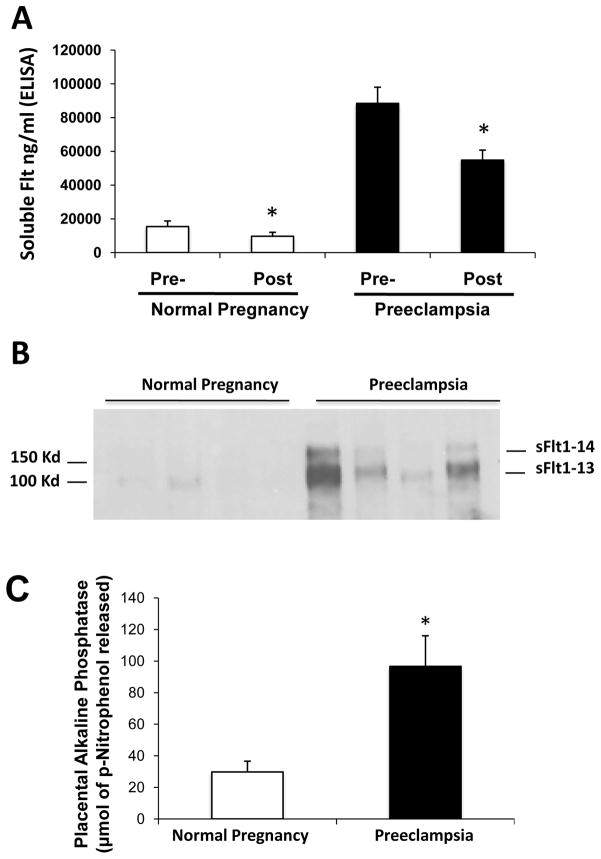
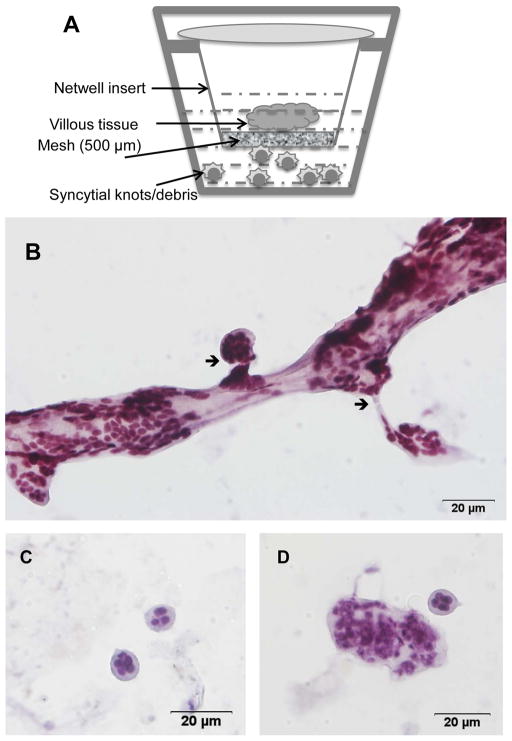
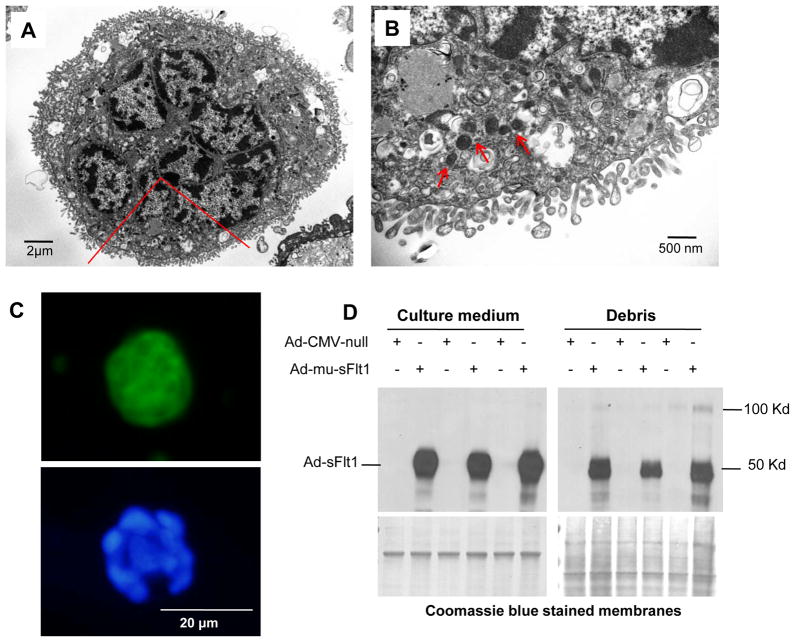
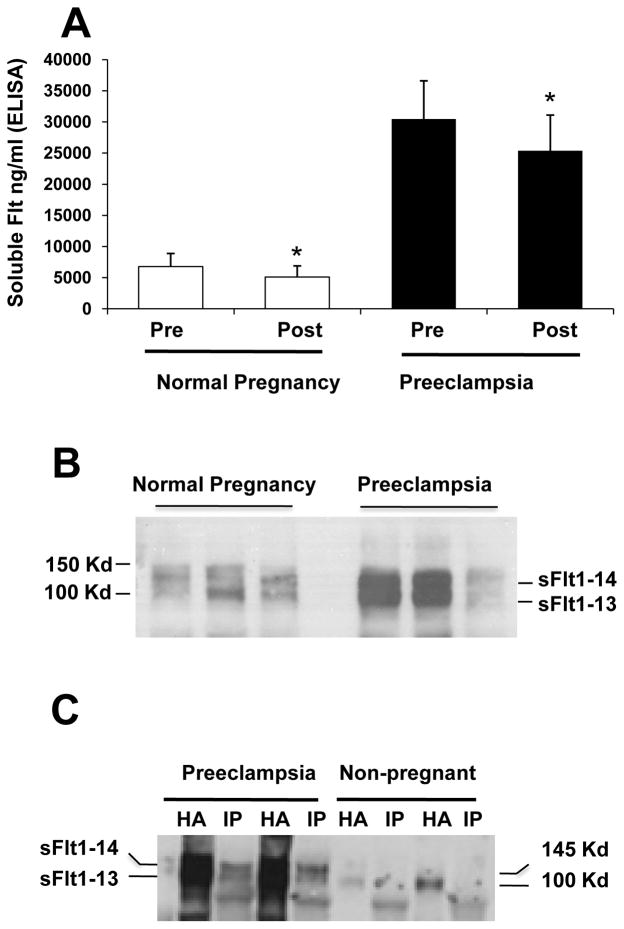
The cardinal manifestations of the pregnancy-specific disorder preeclampsia, new-onset hypertension, and proteinuria that resolve with placental delivery have been linked to an extracellular protein made by the placenta, soluble fms-like tyrosine kinase 1 (sFlt1), that injures the maternal vasculature. However, the mechanisms by which sFlt1, which is heavily matrix bound, gain access to the systemic circulation remain unclear. Here we report that the preeclamptic placenta's outermost layer, the syncytiotrophoblast, forms abundant "knots" that are enriched with sFlt1 protein. These syncytial knots easily detach from the syncytiotrophoblast, resulting in free, multinucleated aggregates (50-150 μm diameter) that are loaded with sFlt1 protein and mRNA, are metabolically active, and are capable of de novo gene transcription and translation. At least 25% of the measurable sFlt1 in the third-trimester maternal plasma is bound to circulating placental microparticles. We conclude that detachment of syncytial knots from the placenta results in free, transcriptionally active syncytial aggregates that represent an autonomous source of sFlt1 delivery into the maternal circulation. The process of syncytial knot formation, shedding of syncytial aggregates, and appearance of placental microparticles in the maternal circulation appears to be greatly accelerated in preeclampsia and may contribute to the maternal vascular injury that characterizes this disorder.
Figures
Comment in
-
Placenta messages to the mother: not just debris.Hypertension. 2012 Feb;59(2):191-3. doi: 10.1161/HYPERTENSIONAHA.111.184861. Epub 2012 Jan 3. Hypertension. 2012. PMID: 22215710 No abstract available.
References
-
- Redman CW, Sargent IL. Latest advances in understanding preeclampsia. Science. 2005;308:1592–1594. - PubMed
-
- Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365:785–799. - PubMed
-
- Ahmad S, Ahmed A. Elevated placental soluble vascular endothelial growth factor receptor-1 inhibits angiogenesis in preeclampsia. Circ Res. 2004;95:884–891. - PubMed
-
- Chaiworapongsa T, Romero R, Espinoza J, Bujold E, Mee Kim Y, Goncalves LF, Gomez R, Edwin S. Evidence supporting a role for blockade of the vascular endothelial growth factor system in the pathophysiology of preeclampsia. Am J Obstet Gynecol. 2004;190:1541–1547. - PubMed
-
- Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, Schisterman EF, Thadhani R, Sachs BP, Epstein FH, Sibai BM, Sukhatme VP, Karumanchi SA. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004;350:672–683. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
