

ROS1 rearrangements define a unique molecular class of lung cancers
- PMID: 22215748
- PMCID: PMC3295572
- DOI: 10.1200/JCO.2011.35.6345
ROS1 rearrangements define a unique molecular class of lung cancers
Abstract
Purpose: Chromosomal rearrangements involving the ROS1 receptor tyrosine kinase gene have recently been described in a subset of non-small-cell lung cancers (NSCLCs). Because little is known about these tumors, we examined the clinical characteristics and treatment outcomes of patients with NSCLC with ROS1 rearrangement.
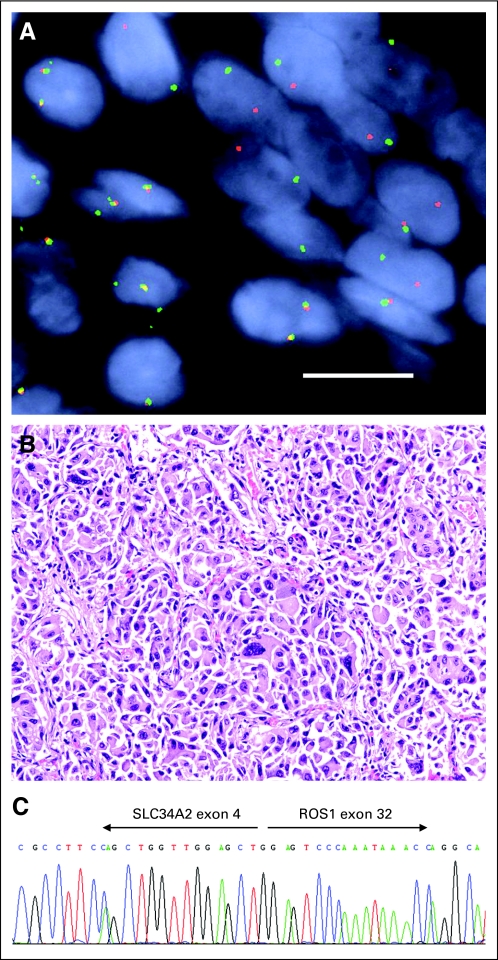
Patients and methods: Using a ROS1 fluorescent in situ hybridization (FISH) assay, we screened 1,073 patients with NSCLC and correlated ROS1 rearrangement status with clinical characteristics, overall survival, and when available, ALK rearrangement status. In vitro studies assessed the responsiveness of cells with ROS1 rearrangement to the tyrosine kinase inhibitor crizotinib. The clinical response of one patient with ROS1-rearranged NSCLC to crizotinib was investigated as part of an expanded phase I cohort.
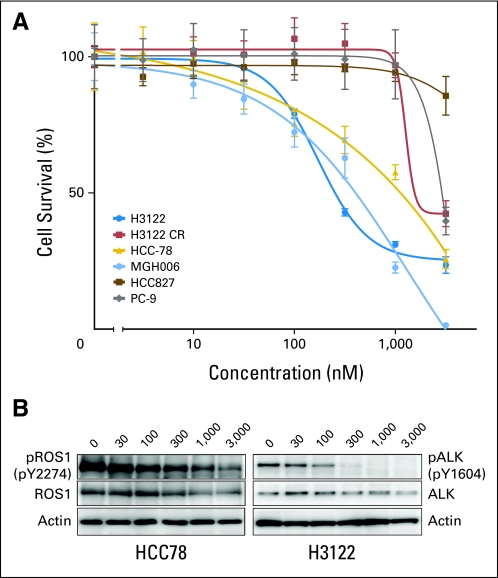
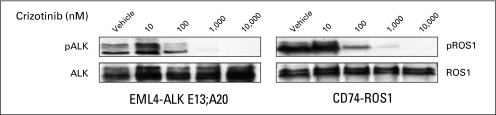
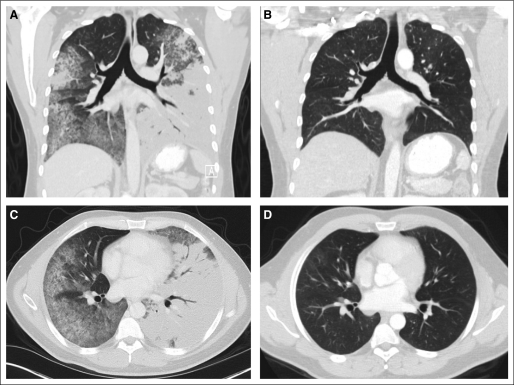
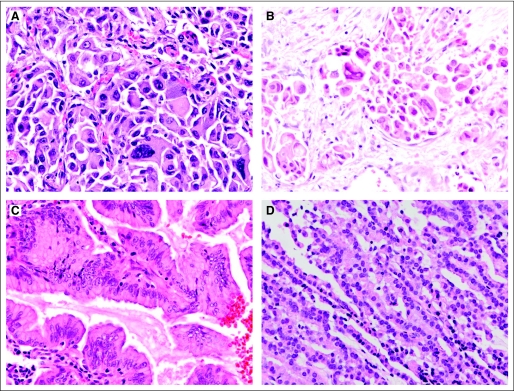
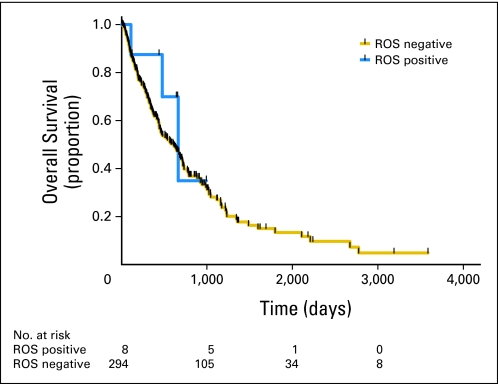
Results: Of 1,073 tumors screened, 18 (1.7%) were ROS1 rearranged by FISH, and 31 (2.9%) were ALK rearranged. Compared with the ROS1-negative group, patients with ROS1 rearrangements were significantly younger and more likely to be never-smokers (each P < .001). All of the ROS1-positive tumors were adenocarcinomas, with a tendency toward higher grade. ROS1-positive and -negative groups showed no difference in overall survival. The HCC78 ROS1-rearranged NSCLC cell line and 293 cells transfected with CD74-ROS1 showed evidence of sensitivity to crizotinib. The patient treated with crizotinib showed tumor shrinkage, with a near complete response.
Conclusion: ROS1 rearrangement defines a molecular subset of NSCLC with distinct clinical characteristics that are similar to those observed in patients with ALK-rearranged NSCLC. Crizotinib shows in vitro activity and early evidence of clinical activity in ROS1-rearranged NSCLC.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
ROS1 rearrangements in lung cancer: a new genomic subset of lung adenocarcinoma.J Clin Oncol. 2012 Mar 10;30(8):878-9. doi: 10.1200/JCO.2011.39.4197. Epub 2012 Jan 3. J Clin Oncol. 2012. PMID: 22215755 No abstract available.
-
HER2 mutations in non-small-cell lung cancer can be continually targeted.J Clin Oncol. 2012 Sep 10;30(26):3318-9. doi: 10.1200/JCO.2012.43.4902. Epub 2012 May 29. J Clin Oncol. 2012. PMID: 22649146 No abstract available.
-
Response to crizotinib in ROS1-rearranged non-small-cell lung cancer.J Clin Oncol. 2012 Sep 20;30(27):3425-6; author reply 3426. doi: 10.1200/JCO.2012.42.4556. Epub 2012 Aug 13. J Clin Oncol. 2012. PMID: 22891268 No abstract available.
References
-
- Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129–2139. - PubMed
-
- Paez JG, Janne PA, Lee JC, et al. EGFR mutations in lung cancer: Correlation with clinical response to gefitinib therapy. Science. 2004;304:1497–1500. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
