

The treatment of central sleep apnea syndromes in adults: practice parameters with an evidence-based literature review and meta-analyses
- PMID: 22215916
- PMCID: PMC3242685
- DOI: 10.5665/sleep.1580
The treatment of central sleep apnea syndromes in adults: practice parameters with an evidence-based literature review and meta-analyses
Abstract
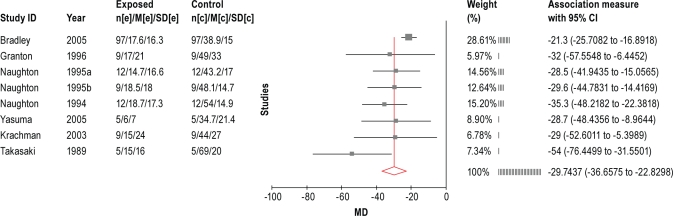
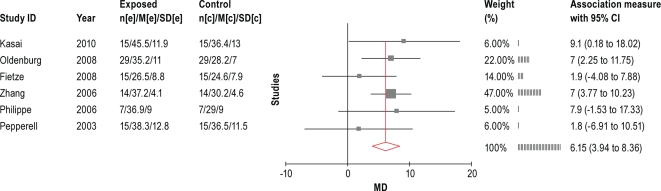
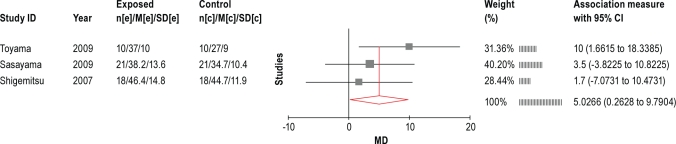
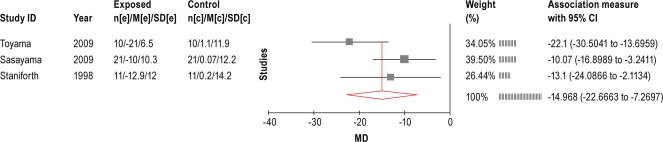
The International Classification of Sleep Disorders, Second Edition (ICSD-2) distinguishes 5 subtypes of central sleep apnea syndromes (CSAS) in adults. Review of the literature suggests that there are two basic mechanisms that trigger central respiratory events: (1) post-hyperventilation central apnea, which may be triggered by a variety of clinical conditions, and (2) central apnea secondary to hypoventilation, which has been described with opioid use. The preponderance of evidence on the treatment of CSAS supports the use of continuous positive airway pressure (CPAP). Much of the evidence comes from investigations on CSAS related to congestive heart failure (CHF), but other subtypes of CSAS appear to respond to CPAP as well. Limited evidence is available to support alternative therapies in CSAS subtypes. The recommendations for treatment of CSAS are summarized as follows: CPAP therapy targeted to normalize the apnea-hypopnea index (AHI) is indicated for the initial treatment of CSAS related to CHF. (STANDARD)Nocturnal oxygen therapy is indicated for the treatment of CSAS related to CHF. (STANDARD)Adaptive Servo-Ventilation (ASV) targeted to normalize the apnea-hypopnea index (AHI) is indicated for the treatment of CSAS related to CHF. (STANDARD)BPAP therapy in a spontaneous timed (ST) mode targeted to normalize the apnea-hypopnea index (AHI) may be considered for the treatment of CSAS related to CHF only if there is no response to adequate trials of CPAP, ASV, and oxygen therapies. (OPTION)The following therapies have limited supporting evidence but may be considered for the treatment of CSAS related to CHF after optimization of standard medical therapy, if PAP therapy is not tolerated, and if accompanied by close clinical follow-up: acetazolamide and theophylline. (OPTION)Positive airway pressure therapy may be considered for the treatment of primary CSAS. (OPTION)Acetazolamide has limited supporting evidence but may be considered for the treatment of primary CSAS. (OPTION)The use of zolpidem and triazolam may be considered for the treatment of primary CSAS only if the patient does not have underlying risk factors for respiratory depression. (OPTION)The following possible treatment options for CSAS related to end-stage renal disease may be considered: CPAP, supplemental oxygen, bicarbonate buffer use during dialysis, and nocturnal dialysis. (OPTION) .
Keywords: ASV; Central sleep apnea; PAP; clinical guidelines; oxygen therapy.
Figures







Comment in
-
Treatment of CSA: a letter to the editor by N.S. Freedman and B.A. Phillips and responses by S. Chowdhuri, et al., on the Task Force report on the Treatment of Adult CSA.Sleep. 2012 Jul 1;35(7):905-7; author reply 905-7. doi: 10.5665/sleep.1948. Sleep. 2012. PMID: 22754036 Free PMC article. No abstract available.
-
Single vs. multi-modality treatment of central apnea syndromes.Sleep. 2012 Sep 1;35(9):1197-8; author reply 1199. doi: 10.5665/sleep.2066. Sleep. 2012. PMID: 22942496 Free PMC article. No abstract available.
References
-
- Balshem H, Helfand M, Schunemann H, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–6. - PubMed
-
- American Academy of Sleep Medicine. International classification of sleep disorders, second edition: diagnostic and coding manual. Westchester, IL: American Academy of Sleep Medicine; 2005.
-
- Mezon B, West P, Israels J, Kryger M. Sleep breathing abnormalities in kyphoscoliosis. Am Rev Respir Dis. 1980;122:617–21. - PubMed
-
- Bitter T, Faber L, et al. Sleep-disordered breathing in heart failure with normal left ventricular ejection fraction. Eur Heart J. 2009;11:602–8. - PubMed
-
- Javaheri S, Parker TJ, Liming JD, et al. Sleep apnea in 81 ambulatory male patients with stable heart failure: types and their prevalences, consequences, and presentations. Circulation. 1998;97:2154–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
