

Prediction of high-grade vesicoureteral reflux after pediatric urinary tract infection: external validation study of procalcitonin-based decision rule
- PMID: 22216314
- PMCID: PMC3247275
- DOI: 10.1371/journal.pone.0029556
Prediction of high-grade vesicoureteral reflux after pediatric urinary tract infection: external validation study of procalcitonin-based decision rule
Erratum in
- PLoS One. 2012 Feb 21;78(8). doi: 10.1371/annotation/c23484a1-f516-4391-a23b-3db456be8edf doi: 10.1371/annotation/c23484a1-f516-4391-a23b-3db456be8edf
Abstract
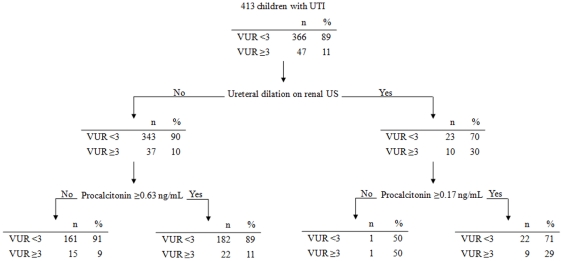
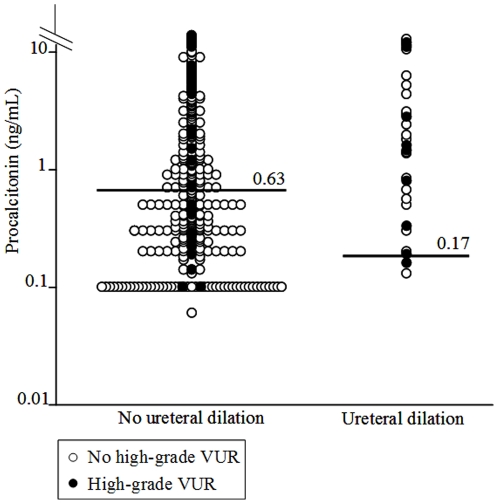
Background: Predicting vesico-ureteral reflux (VUR) ≥3 at the time of the first urinary tract infection (UTI) would make it possible to restrict cystography to high-risk children. We previously derived the following clinical decision rule for that purpose: cystography should be performed in cases with ureteral dilation and a serum procalcitonin level ≥0.17 ng/mL, or without ureteral dilatation when the serum procalcitonin level ≥0.63 ng/mL. The rule yielded a 86% sensitivity with a 46% specificity. We aimed to test its reproducibility.
Study design: A secondary analysis of prospective series of children with a first UTI. The rule was applied, and predictive ability was calculated.
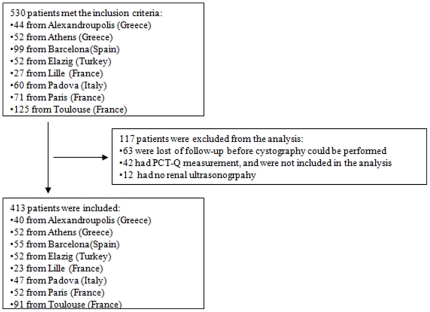
Results: The study included 413 patients (157 boys, VUR ≥3 in 11%) from eight centers in five countries. The rule offered a 46% specificity (95% CI, 41-52), not different from the one in the derivation study. However, the sensitivity significantly decreased to 64% (95%CI, 50-76), leading to a difference of 20% (95%CI, 17-36). In all, 16 (34%) patients among the 47 with VUR ≥3 were misdiagnosed by the rule. This lack of reproducibility might result primarily from a difference between derivation and validation populations regarding inflammatory parameters (CRP, PCT); the validation set samples may have been collected earlier than for the derivation one.
Conclusions: The rule built to predict VUR ≥3 had a stable specificity (ie. 46%), but a decreased sensitivity (ie. 64%) because of the time variability of PCT measurement. Some refinement may be warranted.
© 2011 Leroy et al.
Conflict of interest statement
Figures
References
-
- American Academy of Pediatrics. Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. Pediatrics. 1999;103:843–852. - PubMed
-
- Williams G, Fletcher JT, Alexander SI, Craig JC. Vesicoureteral reflux. J Am Soc Nephrol. 2008;19:847–862. - PubMed
-
- Guignard JP. Urinary infection after micturating cystography. Lancet. 1979;1:103. - PubMed
-
- Garin EH, Olavarria F, Garcia Nieto V, Valenciano B, Campos A, et al. Clinical significance of primary vesicoureteral reflux and urinary antibiotic prophylaxis after acute pyelonephritis: a multicenter, randomized, controlled study. Pediatrics. 2006;117:626–632. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
