

Cardiovascular agents affect the tone of pulmonary arteries and veins in precision-cut lung slices
- PMID: 22216346
- PMCID: PMC3246495
- DOI: 10.1371/journal.pone.0029698
Cardiovascular agents affect the tone of pulmonary arteries and veins in precision-cut lung slices
Abstract
Introduction: Cardiovascular agents are pivotal in the therapy of heart failure. Apart from their action on ventricular contractility and systemic afterload, they affect pulmonary arteries and veins. Although these effects are crucial in heart failure with coexisting pulmonary hypertension or lung oedema, they are poorly defined, especially in pulmonary veins. Therefore, we investigated the pulmonary vascular effects of adrenoceptor agonists, vasopressin and angiotensin II in the model of precision-cut lung slices that allows simultaneous studies of pulmonary arteries and veins.
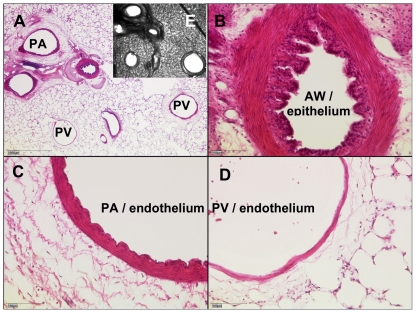
Materials and methods: Precision-cut lung slices were prepared from guinea pigs and imaged by videomicroscopy. Concentration-response curves of cardiovascular drugs were analysed in pulmonary arteries and veins.
Results: Pulmonary veins responded stronger than arteries to α(1)-agonists (contraction) and β(2)-agonists (relaxation). Notably, inhibition of β(2)-adrenoceptors unmasked the α(1)-mimetic effect of norepinephrine and epinephrine in pulmonary veins. Vasopressin and angiotensin II contracted pulmonary veins via V(1a) and AT(1) receptors, respectively, without affecting pulmonary arteries.
Discussion: Vasopressin and (nor)epinephrine in combination with β(2)-inhibition caused pulmonary venoconstriction. If applicable in humans, these treatments would enhance capillary hydrostatic pressures and lung oedema, suggesting their cautious use in left heart failure. Vice versa, the prevention of pulmonary venoconstriction by AT(1) receptor antagonists might contribute to their beneficial effects seen in left heart failure. Further, α(1)-mimetic agents might exacerbate pulmonary hypertension and right ventricular failure by contracting pulmonary arteries, whereas vasopressin might not.
© 2011 Rieg et al.
Conflict of interest statement
Figures
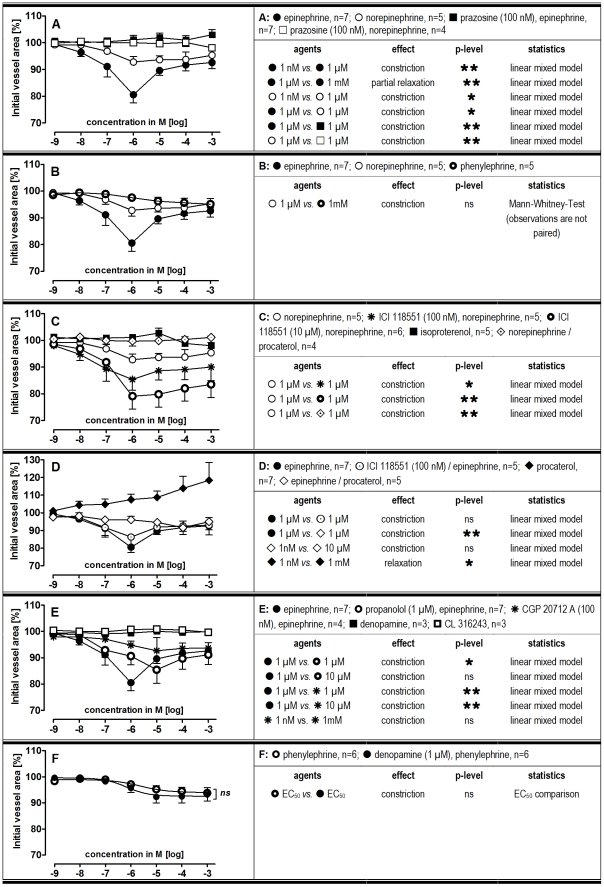
 p<0.05,
p<0.05,  p<0.01 and
p<0.01 and  p<0.001.
p<0.001.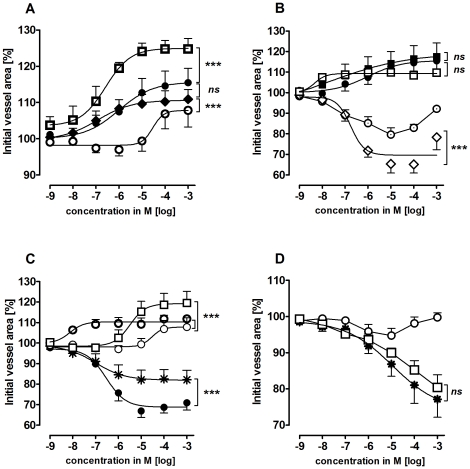
 ) isoproterenol (n = 5); (•) epinephrine (n = 6); (⧫) procaterol (n = 7); (
) isoproterenol (n = 5); (•) epinephrine (n = 6); (⧫) procaterol (n = 7); ( ) norepinephrine (n = 6); B) (•) epinephrine (n = 6); (▪) prazosine (100 nM), epinephrine (n = 6); (
) norepinephrine (n = 6); B) (•) epinephrine (n = 6); (▪) prazosine (100 nM), epinephrine (n = 6); ( ) ICI 118551 (100 nM), epinephrine (n = 5); (⋄) ICI 118551 (10 µM), epinephrine (n = 5); (
) ICI 118551 (100 nM), epinephrine (n = 5); (⋄) ICI 118551 (10 µM), epinephrine (n = 5); ( ) procaterol, epinephrine (n = 4); C) (○) norepinephrine (n = 6); (□) prazosine (100 nM), norepinephrine (n = 3); (
) procaterol, epinephrine (n = 4); C) (○) norepinephrine (n = 6); (□) prazosine (100 nM), norepinephrine (n = 3); ( ) ICI 118551 (100 nM), norepinephrine (n = 9); (•) ICI 118551 (10 µM), norepinephrine (n = 6); (
) ICI 118551 (100 nM), norepinephrine (n = 9); (•) ICI 118551 (10 µM), norepinephrine (n = 6); ( ) procaterol, norepinephrine (n = 4); D) (○) phenylephrine (n = 6); (
) procaterol, norepinephrine (n = 4); D) (○) phenylephrine (n = 6); ( ) A 61603 (n = 5), (□) ICI 118551 (100 nM), phenylephrine (n = 5). Asterics indicate different EC50.values of the various curves. P<0.05 are considered as statistical significant and are indicated as followed
) A 61603 (n = 5), (□) ICI 118551 (100 nM), phenylephrine (n = 5). Asterics indicate different EC50.values of the various curves. P<0.05 are considered as statistical significant and are indicated as followed  p<0.05,
p<0.05,  p<0.01 and
p<0.01 and  p<0.001.
p<0.001.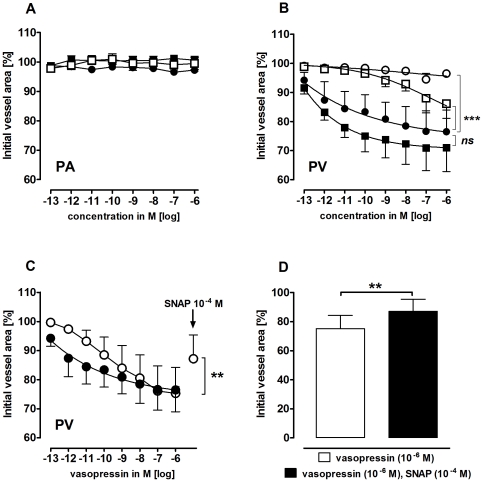
 ) indomethacin (10 µM), vasopressin (n = 4); (▪) L-NAME (100 µM), vasopressin (n = 5) B) PV: (•) vasopressin (n = 5); (
) indomethacin (10 µM), vasopressin (n = 4); (▪) L-NAME (100 µM), vasopressin (n = 5) B) PV: (•) vasopressin (n = 5); ( ) indomethacin (10 µM), vasopressin (n = 4); (▪) L-NAME (100 µM), vasopressin (n = 5); (
) indomethacin (10 µM), vasopressin (n = 4); (▪) L-NAME (100 µM), vasopressin (n = 5); ( ) SR 49059 (10 nM), vasopressin (n = 3). C) PV: (•) vasopressin (n = 5); (
) SR 49059 (10 nM), vasopressin (n = 3). C) PV: (•) vasopressin (n = 5); ( ) vasopressin, SNAP (n = 7). D) PV: vasopressin, SNAP (n = 7). B) Asterics indicate different EC50.values of the various curves. C–D) Statistics was performed using the Wilcoxon test. For all: P<0.05 are considered as statistical significant and are indicated as followed
) vasopressin, SNAP (n = 7). D) PV: vasopressin, SNAP (n = 7). B) Asterics indicate different EC50.values of the various curves. C–D) Statistics was performed using the Wilcoxon test. For all: P<0.05 are considered as statistical significant and are indicated as followed  p<0.05,
p<0.05,  p<0.01 and
p<0.01 and  p<0.001.
p<0.001.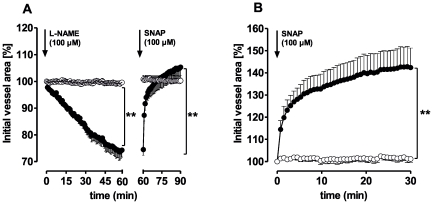
 p<0.05,
p<0.05,  p<0.01 and
p<0.01 and  p<0.001.
p<0.001.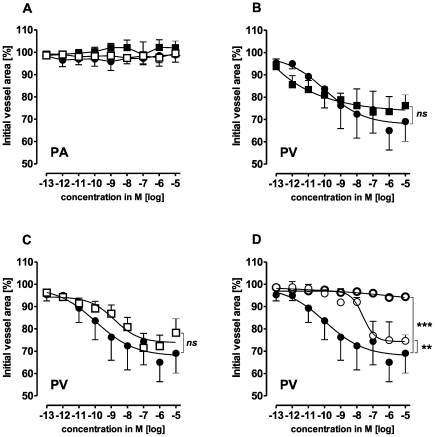
 ) indomethacin (10 µM), angiotensin II (n = 5); (▪) L-NAME (100 µM), angiotensin II (n = 5) B) PV: (•) angiotensin II (n = 5); (▪) L-NAME (100 µM), angiotensin II (n = 5) C) PV: (•) angiotensin II (n = 5); (
) indomethacin (10 µM), angiotensin II (n = 5); (▪) L-NAME (100 µM), angiotensin II (n = 5) B) PV: (•) angiotensin II (n = 5); (▪) L-NAME (100 µM), angiotensin II (n = 5) C) PV: (•) angiotensin II (n = 5); ( ) indomethacin (10 µM), angiotensin II (n = 5) D) PV: (•) angiotensin II (n = 5); (
) indomethacin (10 µM), angiotensin II (n = 5) D) PV: (•) angiotensin II (n = 5); ( ) losartan (1 µM), angiotensin II (n = 3); (○) losartan (10 nM), angiotensin II (n = 3). Asterics indicate different EC50.values of the various curves. P<0.05 are considered as statistical significant and are indicated as followed
) losartan (1 µM), angiotensin II (n = 3); (○) losartan (10 nM), angiotensin II (n = 3). Asterics indicate different EC50.values of the various curves. P<0.05 are considered as statistical significant and are indicated as followed  p<0.05,
p<0.05,  p<0.01 and
p<0.01 and  p<0.001.
p<0.001.Similar articles
-
Levosimendan Relaxes Pulmonary Arteries and Veins in Precision-Cut Lung Slices - The Role of KATP-Channels, cAMP and cGMP.PLoS One. 2013 Jun 18;8(6):e66195. doi: 10.1371/journal.pone.0066195. Print 2013. PLoS One. 2013. PMID: 23824760 Free PMC article.
-
Differential relaxant responses of pulmonary arteries and veins in lung explants of guinea pigs.J Appl Physiol (1985). 1997 Nov;83(5):1476-81. doi: 10.1152/jappl.1997.83.5.1476. J Appl Physiol (1985). 1997. PMID: 9375308
-
Tyrosine kinase inhibitors relax pulmonary arteries in human and murine precision-cut lung slices.Respir Res. 2019 Jun 6;20(1):111. doi: 10.1186/s12931-019-1074-2. Respir Res. 2019. PMID: 31170998 Free PMC article.
-
Modulation of vascular tone and reactivity by nitric oxide in porcine pulmonary arteries and veins.Acta Physiol Scand. 2002 Jan;174(1):9-15. doi: 10.1046/j.1365-201x.2002.00928.x. Acta Physiol Scand. 2002. PMID: 11851592
-
Imatinib relaxes the pulmonary venous bed of guinea pigs.Respir Res. 2017 Feb 8;18(1):32. doi: 10.1186/s12931-017-0514-0. Respir Res. 2017. PMID: 28178968 Free PMC article.
Cited by
-
Precision cut lung slices: an integrated ex vivo model for studying lung physiology, pharmacology, disease pathogenesis and drug discovery.Respir Res. 2024 Jun 1;25(1):231. doi: 10.1186/s12931-024-02855-6. Respir Res. 2024. PMID: 38824592 Free PMC article. Review.
-
Diallylthiosulfinate (Allicin), a Volatile Antimicrobial from Garlic (Allium sativum), Kills Human Lung Pathogenic Bacteria, Including MDR Strains, as a Vapor.Molecules. 2017 Oct 12;22(10):1711. doi: 10.3390/molecules22101711. Molecules. 2017. PMID: 29023413 Free PMC article.
-
Evaluation of inflammatory and immune responses in long-term cultured human precision-cut lung slices.Hum Vaccin Immunother. 2017 Feb;13(2):351-358. doi: 10.1080/21645515.2017.1264794. Hum Vaccin Immunother. 2017. PMID: 27929748 Free PMC article.
-
Different Effects of Riociguat and Vericiguat on Pulmonary Vessels and Airways.Biomedicines. 2025 Apr 2;13(4):856. doi: 10.3390/biomedicines13040856. Biomedicines. 2025. PMID: 40299433 Free PMC article.
-
Levosimendan Relaxes Pulmonary Arteries and Veins in Precision-Cut Lung Slices - The Role of KATP-Channels, cAMP and cGMP.PLoS One. 2013 Jun 18;8(6):e66195. doi: 10.1371/journal.pone.0066195. Print 2013. PLoS One. 2013. PMID: 23824760 Free PMC article.
References
-
- Evora P, Pearson P, Schaff H. Arginine vasopressin induces endothelium-dependent vasodilatation of the pulmonary artery. V1-receptor-mediated production of nitric oxide. Chest. 1993;103:1241–1245. - PubMed
-
- Leather H, Segers P, Berends N, Vandermeersch E, Wouters P. Effects of vasopressin on right ventricular function in an experimental model of acute pulmonary hypertension. Crit Care Med. 2002;30:2548–2552. - PubMed
-
- Russ R, Resta T, Walker B. Pulmonary vasodilatory response to neurohypophyseal peptides in the rat. J Appl Physiol. 1992;73:473–478. - PubMed
-
- Sai Y, Okamura T, Amakata Y, Toda N. Comparison of responses of canine pulmonary artery and vein to angiotensin II, bradykinin and vasopressin. Eur J Pharmacol. 1995;282:235–241. - PubMed
-
- Uma S, Tuncer M. Beta-adrenoceptor stimulating effects of phenylephrine and noradrenaline in the rat pulmonary vascular bed. J Pharm Pharmacol. 1988;40:219–220. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
