

Shining a light on xeroderma pigmentosum
- PMID: 22217736
- PMCID: PMC3279615
- DOI: 10.1038/jid.2011.426
Shining a light on xeroderma pigmentosum
Abstract
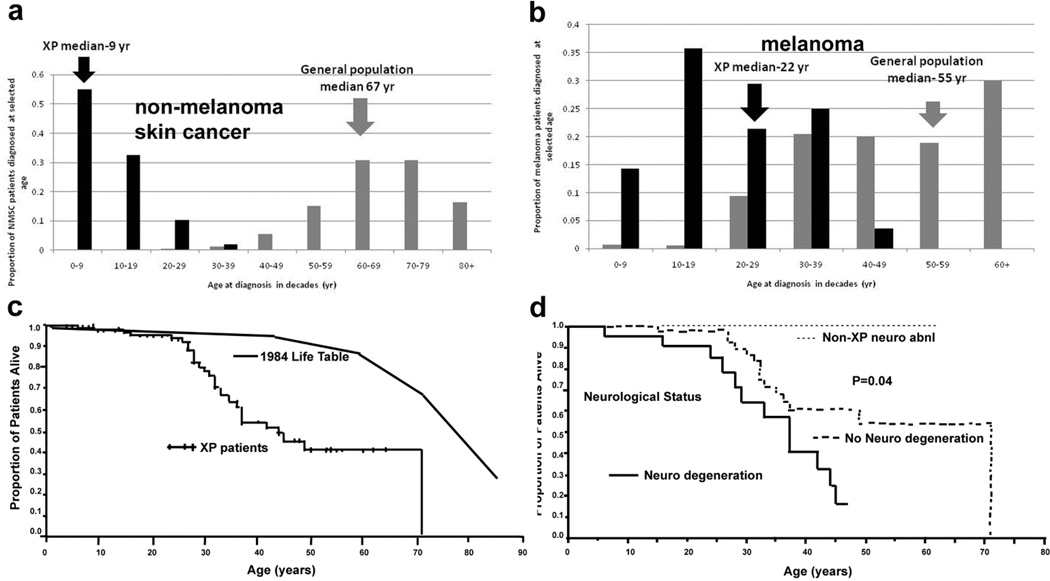
Xeroderma pigmentosum (XP) is a rare, autosomal recessive disorder of DNA repair characterized by sun sensitivity and UV radiation-induced skin and mucous membrane cancers. Initially described in 1874 by Moriz Kaposi in Vienna, nearly 100 years later, James Cleaver in San Francisco reported defective DNA repair in XP cells. This eventually provided the basis for a mechanistic link between sun exposure, DNA damage, somatic mutations, and skin cancer. XP cells were found to have defects in seven of the proteins of the nucleotide excision repair pathway and in DNA polymerase η. XP cells are hypersensitive to killing by UV radiation, and XP cancers have characteristic "UV signature" mutations. Clinical studies at the National Institutes of Health found a nearly 10,000-fold increase in skin cancer in XP patients under the age of 20 years, demonstrating the substantial importance of DNA repair in cancer prevention in the general population. Approximately 25% of XP patients have progressive neurological degeneration with progressive loss of neurons, probably from DNA damage induced by oxidative metabolism, which kills nondividing cells in the nervous system. Interestingly, patients with another disorder, trichothiodystrophy, have defects in some of the same genes as XP, but they have primary developmental abnormalities without an increase in skin cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Alekseev S, Kool H, Rebel H, Fousteri M, Moser J, Backendorf C, et al. Enhanced DDB2 expression protects mice from carcinogenic effects of chronic UV-B irradiation. Cancer Res. 2005;65(22):10298–10306. - PubMed
-
- Arase S, Kozuka T, Tanaka K, Ikenaga M, Takebe H. A sixth complementation group in xeroderma pigmentosum. Mutat.Res. 1979;59:143–146. - PubMed
-
- Blankenburg S, Konig IR, Moessner R, Laspe P, Thoms KM, Krueger U, et al. Assessment of 3 xeroderma pigmentosum group C gene polymorphisms and risk of cutaneous melanoma: a case-control study. Carcinogenesis. 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
