

Health span approximates life span among many supercentenarians: compression of morbidity at the approximate limit of life span
- PMID: 22219514
- PMCID: PMC3309876
- DOI: 10.1093/gerona/glr223
Health span approximates life span among many supercentenarians: compression of morbidity at the approximate limit of life span
Abstract
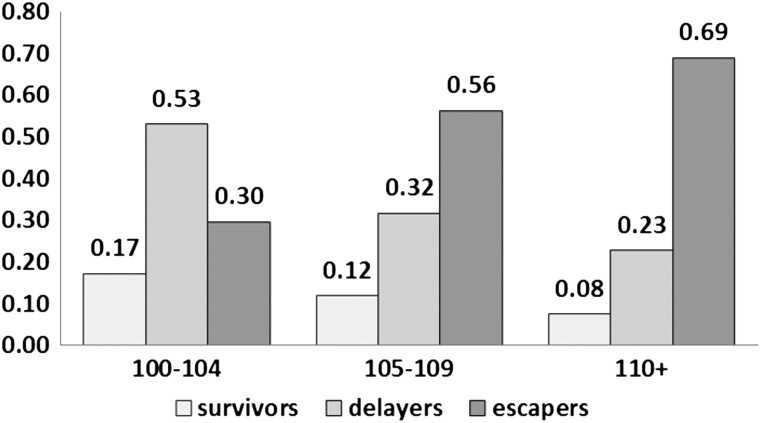
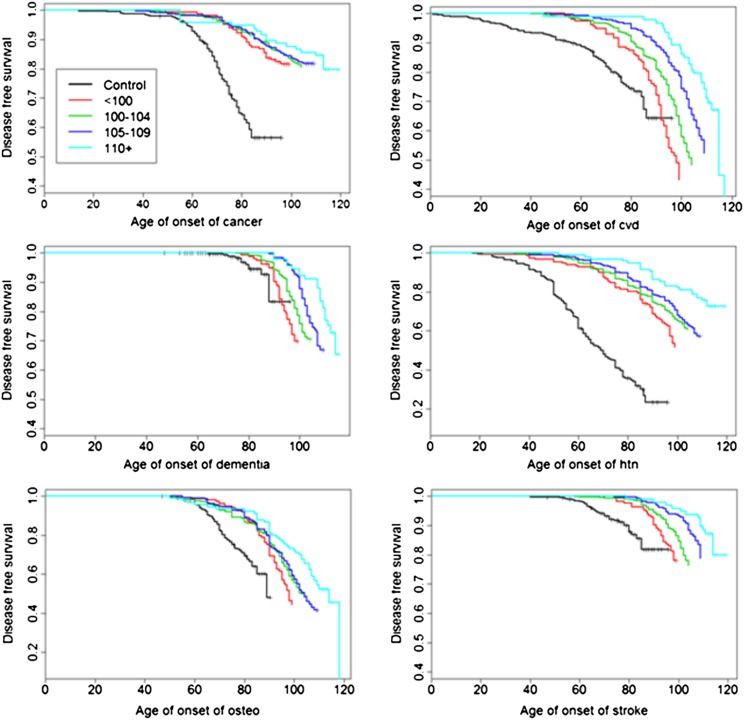
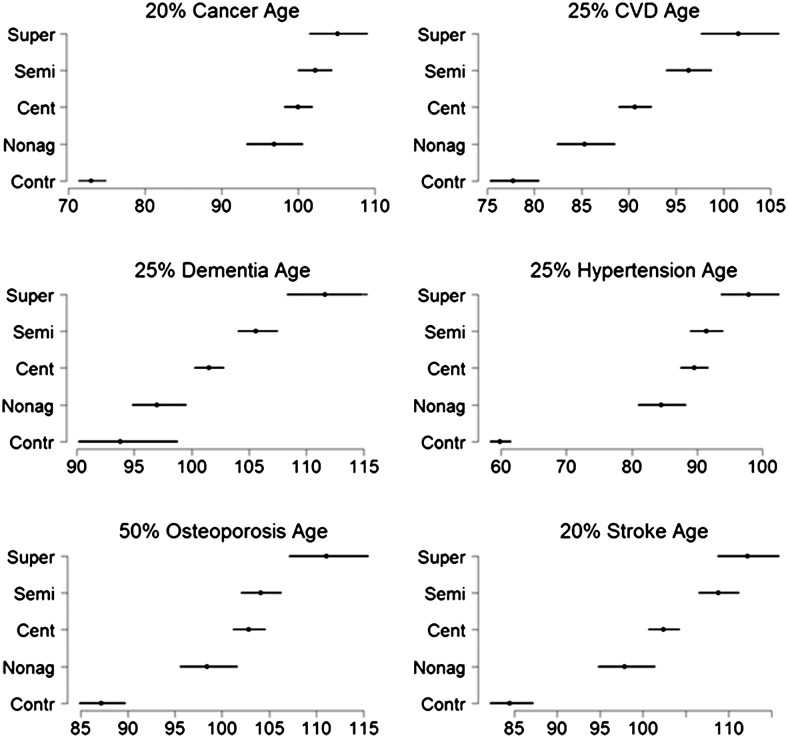
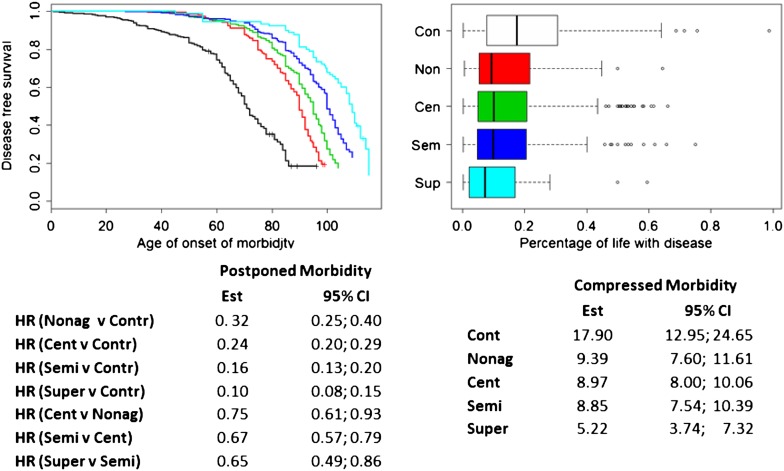
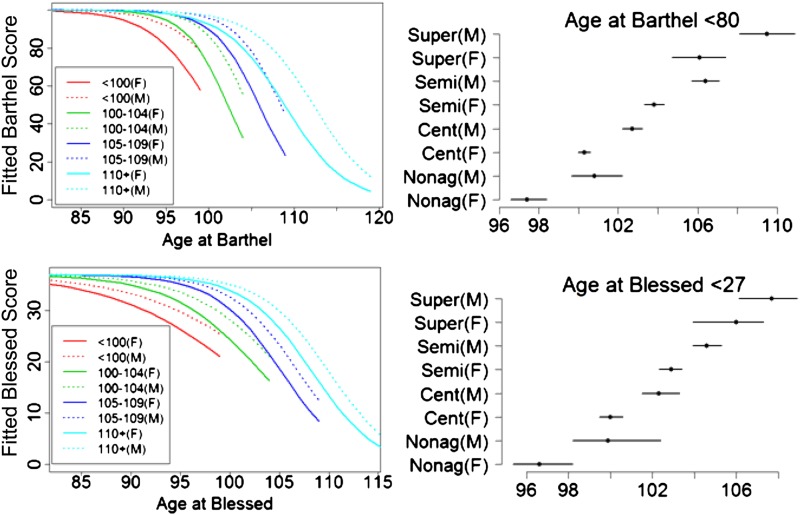
We analyze the relationship between age of survival, morbidity, and disability among centenarians (age 100-104 years), semisupercentenarians (age 105-109 years), and supercentenarians (age 110-119 years). One hundred and four supercentenarians, 430 semisupercentenarians, 884 centenarians, 343 nonagenarians, and 436 controls were prospectively followed for an average of 3 years (range 0-13 years). The older the age group, generally, the later the onset of diseases, such as cancer, cardiovascular disease, dementia, and stroke, as well as of cognitive and functional decline. The hazard ratios for these individual diseases became progressively less with older and older age, and the relative period of time spent with disease was lower with increasing age group. We observed a progressive delay in the age of onset of physical and cognitive function impairment, age-related diseases, and overall morbidity with increasing age. As the limit of human life span was effectively approached with supercentenarians, compression of morbidity was generally observed.
Figures
References
-
- Young RD, Desjardins B, McLaughlin K, Poulain M, Perls T. Typologies of extreme longevity myths. Curr Gerontol Geriatr Res. 2011:1–12. http://www.hindawi.com/journals/cggr/2010/423087/Accessed December 1, 2011. - PMC - PubMed
-
- Kestenbaum B, Ferguson RB. Number of centenarians in the United States Jan. 1, 1990, 2000 and 2010 based on improved medicare data. N Am Actuar J. 2005;10:1–6. http://ccp.ucr.ac.cr/creles/100m/m-rs05-1_xxvi.pdf. Accessed December 1, 2011.
-
- Bell FC, Miller ML. Life Tables for the United States Social Security Area 1900–2100, Actuarial Study No. 120. 2005. http://www.ssa.gov/oact/NOTES/as120/LifeTables_Tbl_7_1900.html. Accessed September 5, 2011.
-
- Bourbeau R. Demography. Tracking Down Supercentenarians. Universite de Montreal Research Bulletin; 2002. http://www.forum.umontreal.ca/forum_express/pages_a/demo.htmAccessed December 11, 2011.
-
- Robine JM, Allard M. The oldest human. Science. 1998;279:1834–1835. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
