

Early mortality in adults initiating antiretroviral therapy (ART) in low- and middle-income countries (LMIC): a systematic review and meta-analysis
- PMID: 22220193
- PMCID: PMC3248405
- DOI: 10.1371/journal.pone.0028691
Early mortality in adults initiating antiretroviral therapy (ART) in low- and middle-income countries (LMIC): a systematic review and meta-analysis
Abstract
Background: We systematically reviewed observational studies of early mortality post-antiretroviral therapy (ART) initiation in low- and middle-income countries (LMIC) in Asia, Africa, and Central and South America, as defined by the World Bank, to summarize what is known.
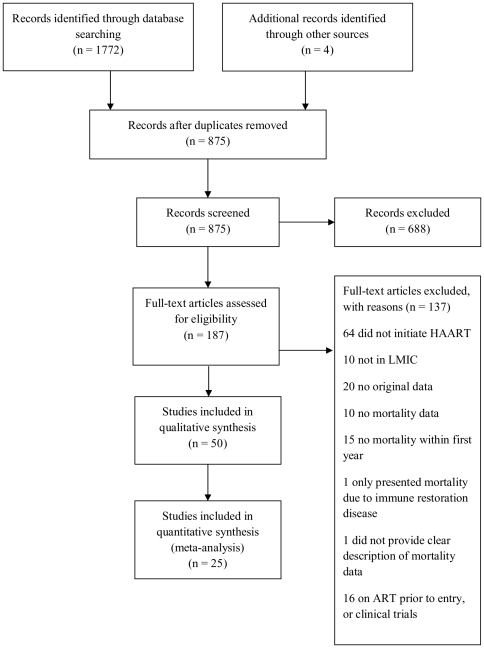
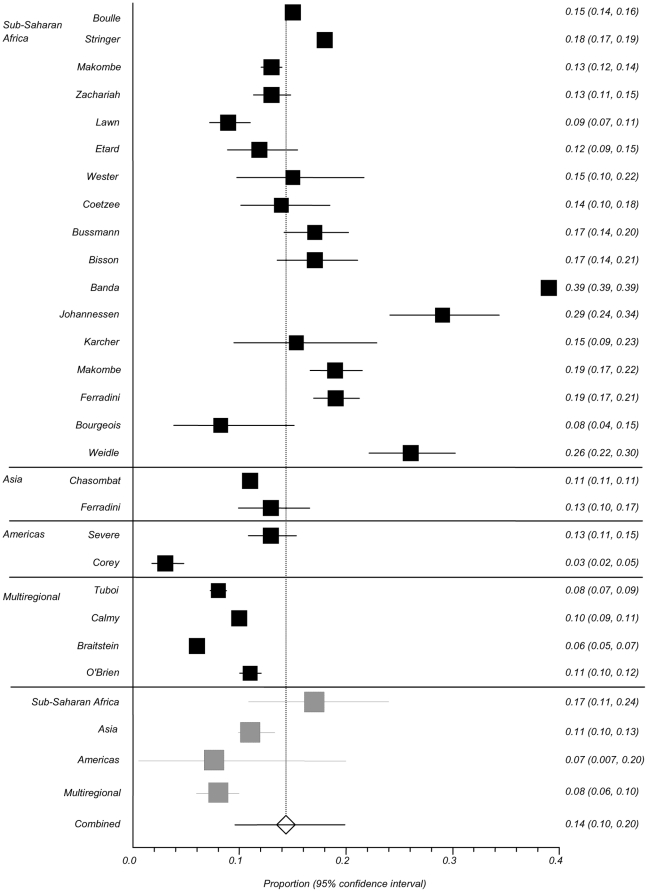
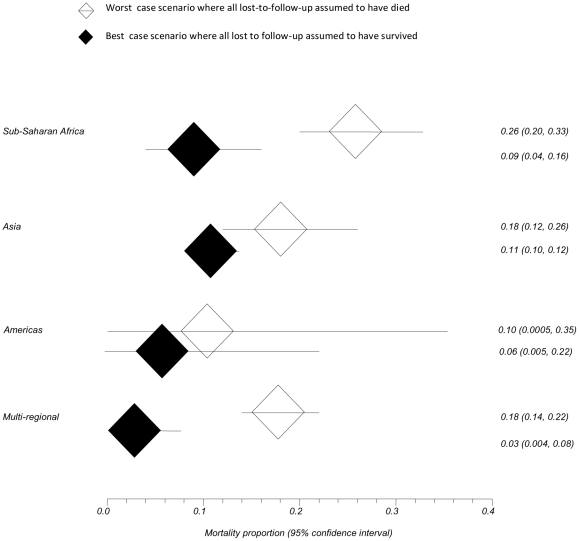
Methods and findings: Studies published in English between January 1996 and December 2010 were searched in Medline and EMBASE. Three independent reviewers examined studies of mortality within one year post-ART. An article was included if the study was conducted in a LMIC, participants were initiating ART in a non-clinical trial setting and were ≥15 years. Fifty studies were included; 38 (76%) from sub-Saharan Africa (SSA), 5 (10%) from Asia, 2 (4%) from the Americas, and 5 (10%) were multi-regional. Median follow-up time and pre-ART CD4 cell count ranged from 3-55 months and 11-192 cells/mm(3), respectively. Loss-to-follow-up, reported in 40 (80%) studies, ranged from 0.3%-27%. Overall, SSA had the highest pooled 12-month mortality probability of 0.17 (95% CI 0.11-0.24) versus 0.11 (95% CI 0.10-0.13) for Asia, and 0.07 (95% CI 0.007-0.20) for the Americas. Of 14 (28%) studies reporting cause-specific mortality, tuberculosis (TB) (5%-44%), wasting (5%-53%), advanced HIV (20%-37%), and chronic diarrhea (10%-25%) were most common. Independent factors associated with early mortality in 30 (60%) studies included: low baseline CD4 cell count, male sex, advanced World Health Organization clinical stage, low body mass index, anemia, age greater than 40 years, and pre-ART quantitative HIV RNA.
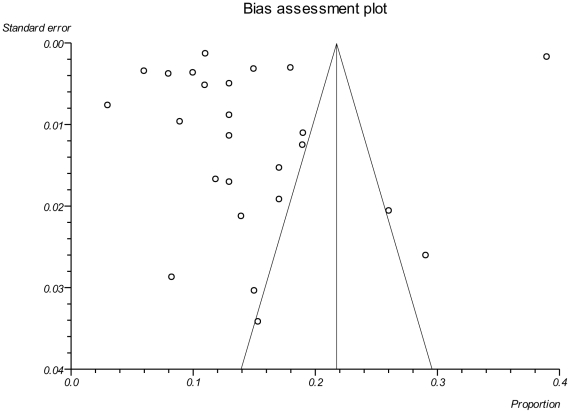
Conclusions: Significant heterogeneity in outcomes and in methods of reporting outcomes exist among published studies evaluating mortality in the first year after ART initiation in LMIC. Early mortality rates are highest in SSA, and opportunistic illnesses such as TB and wasting syndrome are the most common reported causes of death. Strategies addressing modifiable risk factors associated with early death are urgently needed.
Conflict of interest statement
Figures
References
-
- Joint United Nations Programme on HIV and AIDS (UNAIDS) Financial Resources Required to Achieve, Universal Access to HIV Prevention, Treatment Care and Support. 2007. Available: http://data.unaids.org/pub/Report/2007/JC1678_Fin_Res_Req_en.pdf.
-
- Palella FJ, Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. - PubMed
-
- Severe P, Leger P, Charles M, Noel F, Bonhomme G, et al. Antiretroviral therapy in a thousand patients with AIDS in Haiti. N Engl J Med. 2005;353:2325–2334. - PubMed
-
- Stringer JS, Zulu I, Levy J, Stringer EM, Mwango A, et al. Rapid scale-up of antiretroviral therapy at primary care sites in Zambia: feasibility and early outcomes. JAMA. 2006;296:782–793. - PubMed
-
- Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–824. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
