

Growth in the use of PET for six cancer types after coverage by medicare: additive or replacement?
- PMID: 22221634
- PMCID: PMC3257824
- DOI: 10.1016/j.jacr.2011.06.019
Growth in the use of PET for six cancer types after coverage by medicare: additive or replacement?
Abstract
Background: In July 2001, PET became a covered service for Medicare beneficiaries when used for the diagnosis, staging, and restaging of non-small-cell lung, esophageal, colorectal, and head and neck cancers as well as lymphoma and melanoma. Whether physicians use PET as a replacement for or in addition to CT, MRI, or bone scintigraphy (BS) is uncertain.
Methods: A 20% sample of Medicare fee-for-service beneficiaries aged > 64 years from 2004 through 2008 was used. Annually for each cancer type, a cohort of patients was created defined as having at least one admission with a primary cancer diagnosis or two nonhospital claims with a cancer diagnosis ≥7 days apart per calendar year. Each year, imaging claims and claim-days were counted by modality and cancer type. The sequence of PET use was examined as before, after, or instead of other imaging.
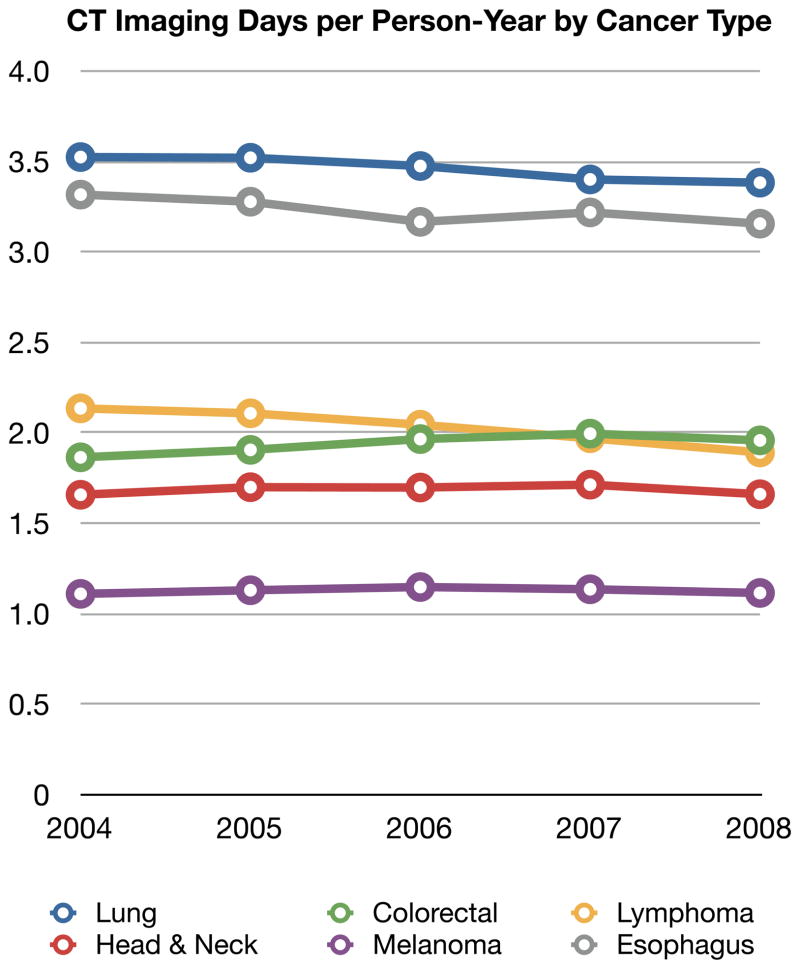
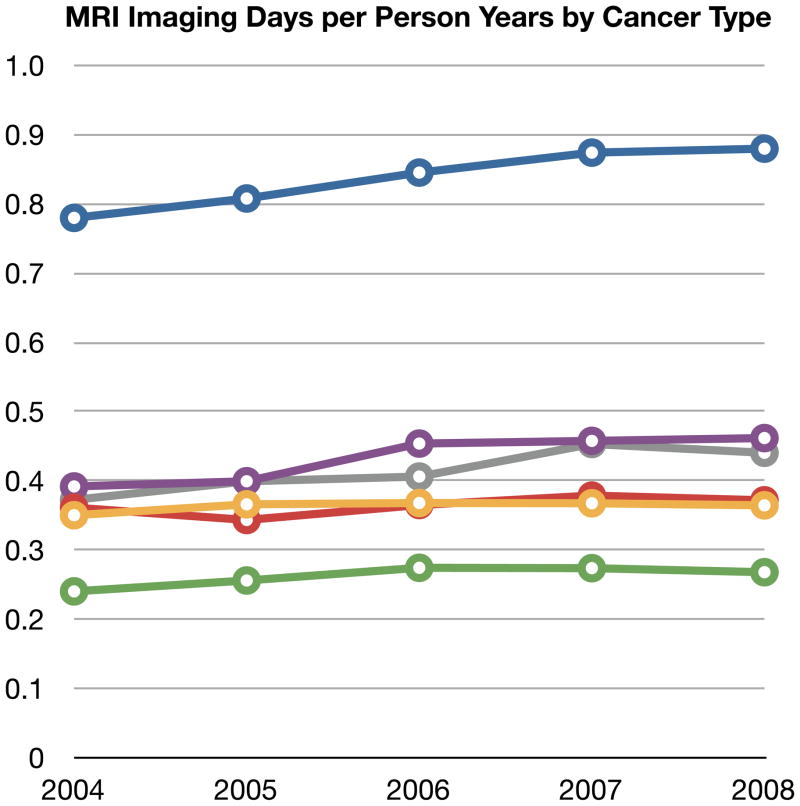
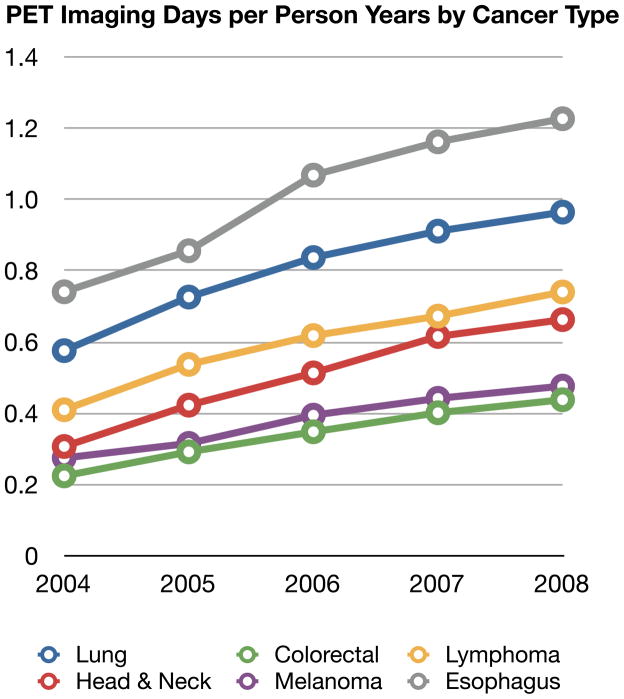
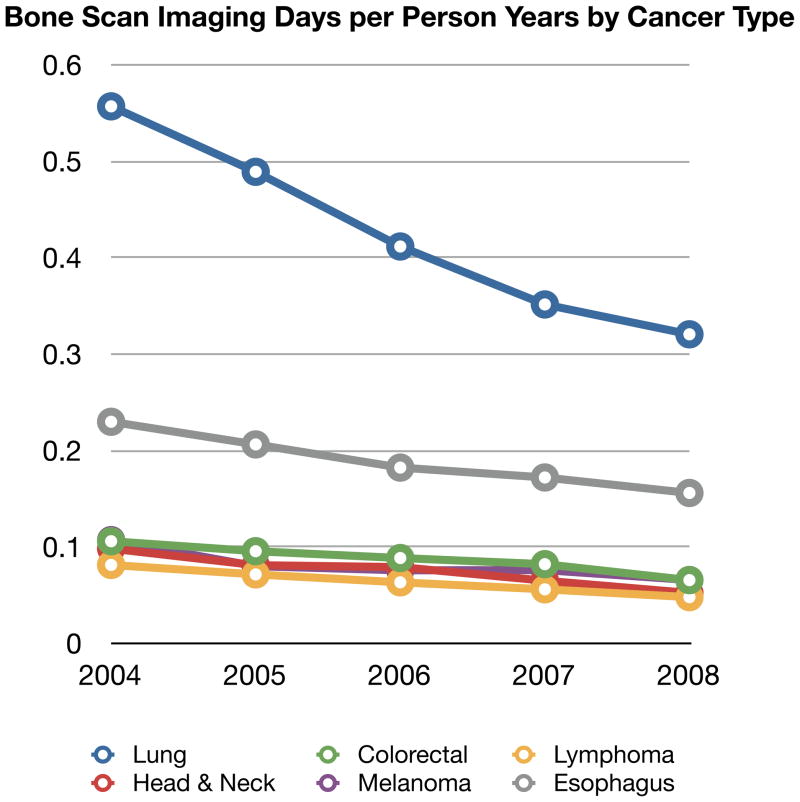
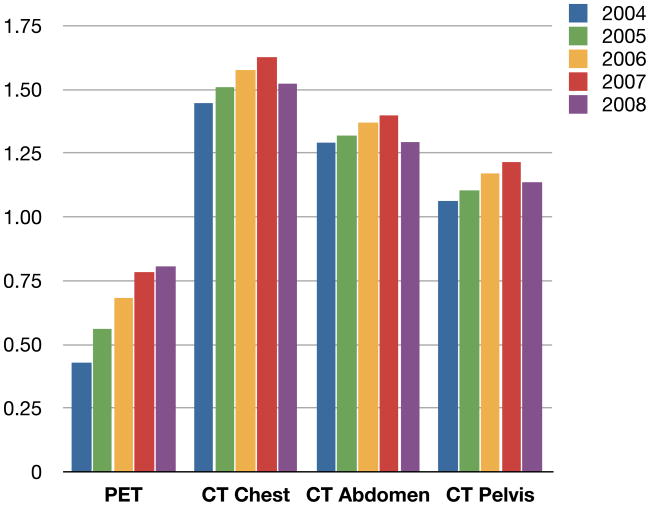
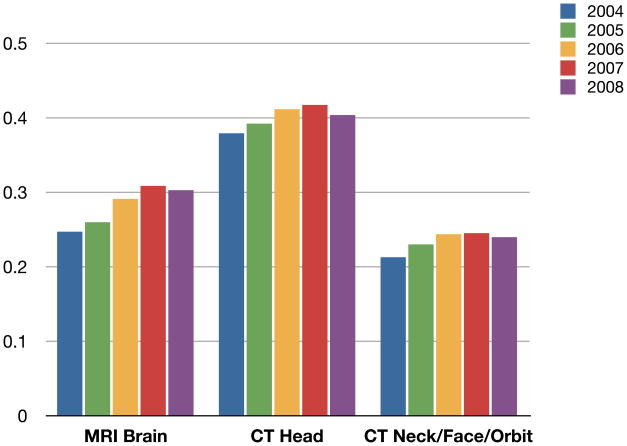
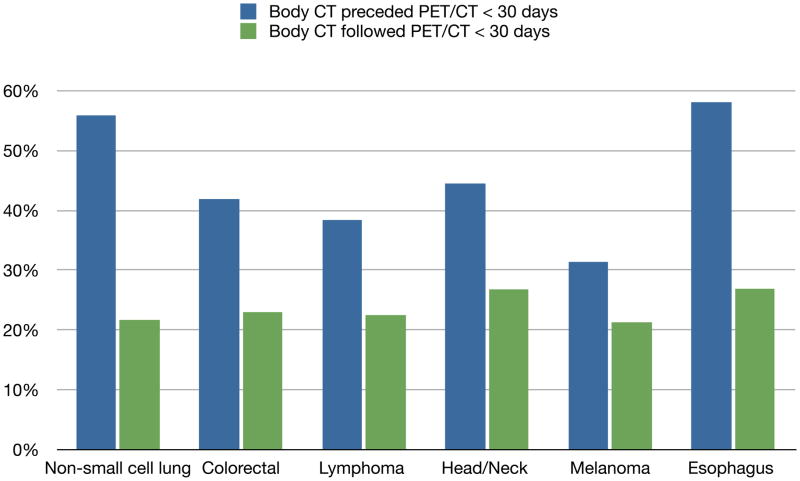
Results: About 125,000 beneficiaries (2.5% of the cohort) met the cancer definition each year. In 2008, the combined annual imaging days per person-year were 2.3 for CT, 0.49 for MRI, 0.70 for PET, and 0.13 for BS. The annual rates of imaging from 2004 to 2008 increased by 0.5% for CT, 3.2% for MRI, and 18.0% for PET (range, 14.6%-19.9% by cancer type) and decreased by 12.7% for BS. The growth in PET use was not associated with meaningful changes in body CT. In 2007 and 2008, body CT preceded PET within 30 days in about half of patients, whereas PET preceded CT in only 22%.
Conclusions: Several years after its introduction, PET continued to grow rapidly, with evidence that it is replacing BS. Growth of PET occurred without evidence of a decline in body CT. About half of PET use occurred shortly after body CT, suggesting an additive or final arbiter role.
Copyright © 2012 American College of Radiology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- National Comprehensive Cancer Network. [Accessed (December 27, 2010];NCCN Guidelines ™. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp-site.
-
- American College of Radiology. [(Accessed January 2, 2011)];ACR Appropriateness Criteria®. http://www.acr.org/secondarymainmenucategories/quality_safety/app_criter....
-
- Podoloff DA, Ball DW, Ben-Josef E, et al. NCCN task force: clinical utility of PET in a variety of tumor types. J Natl Compr Canc Netw. 2009;7 (Suppl 2):S1–26. - PubMed
-
- Meropol NJ, Schrag D, Smith TJ, et al. American Society of Clinical Oncology Guidance Statement: The Cost of Cancer Care. J Clin Oncol. 2009;27:3868–74. - PubMed
-
- Levin DC, Rao VM, Parker L, Frangos AJ. The Disproportionate Effects of the Deficit Reduction Act of 2005 on Radiologists’ Private Office MRI and CT Practices Compared With Those of Other Physicians. J Am Coll Radiol. 2009;6:620–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
