

Hyponatremia, hypernatremia, and mortality in patients with chronic kidney disease with and without congestive heart failure
- PMID: 22223429
- PMCID: PMC3294276
- DOI: 10.1161/CIRCULATIONAHA.111.065391
Hyponatremia, hypernatremia, and mortality in patients with chronic kidney disease with and without congestive heart failure
Abstract
Background: Hyponatremia is common in patients with conditions such as congestive heart failure and is associated with increased mortality in hospitalized patients. Congestive heart failure is common in patients with chronic kidney disease, but the association of serum sodium concentration with mortality in such patients is not well characterized.
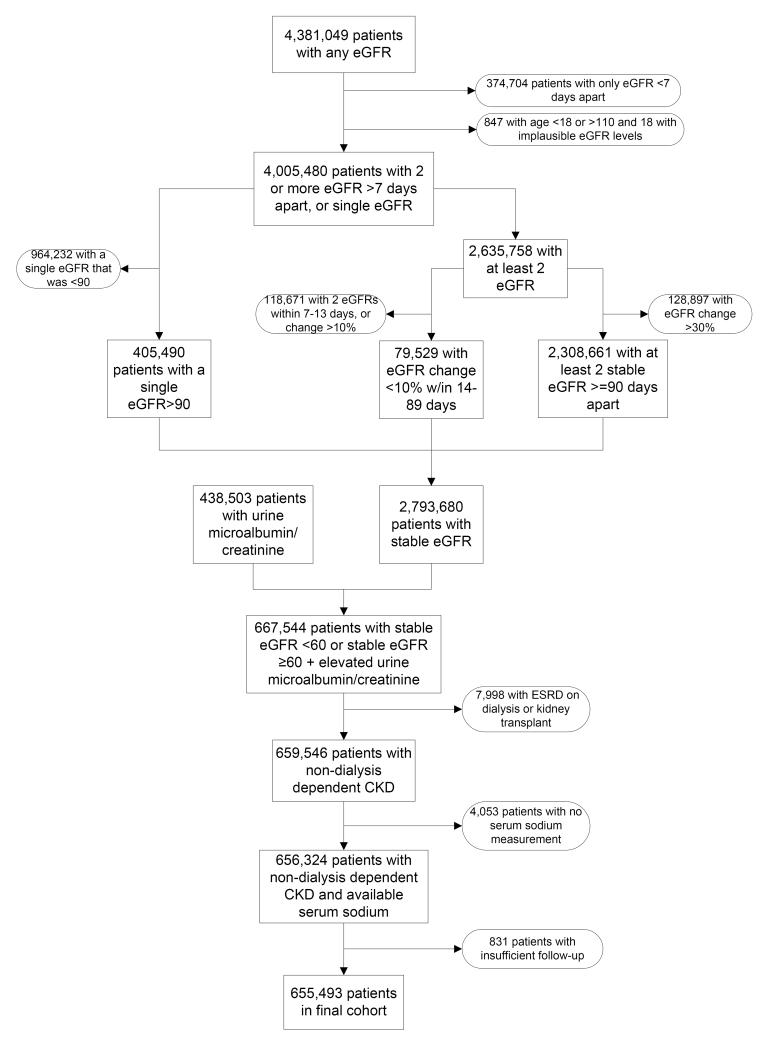
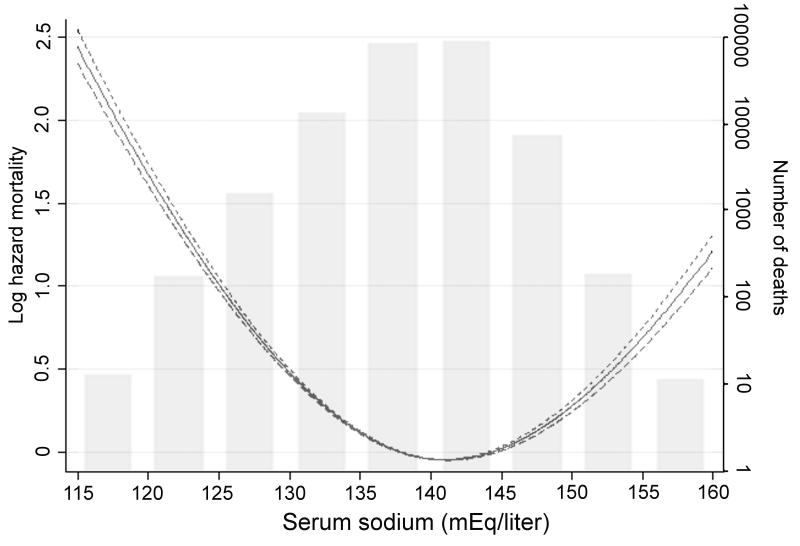
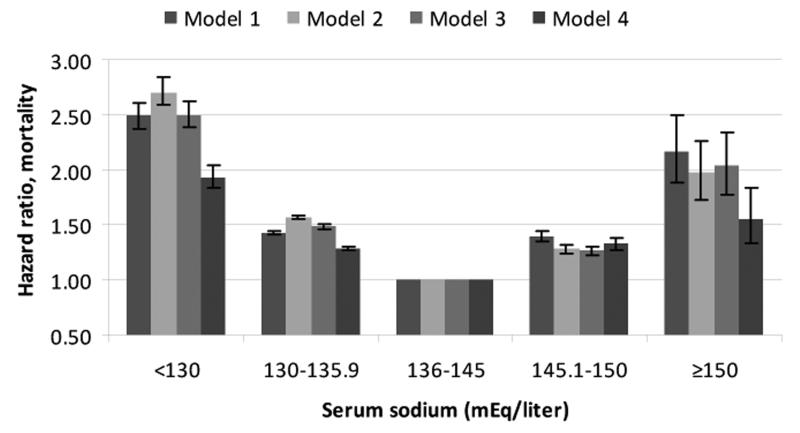
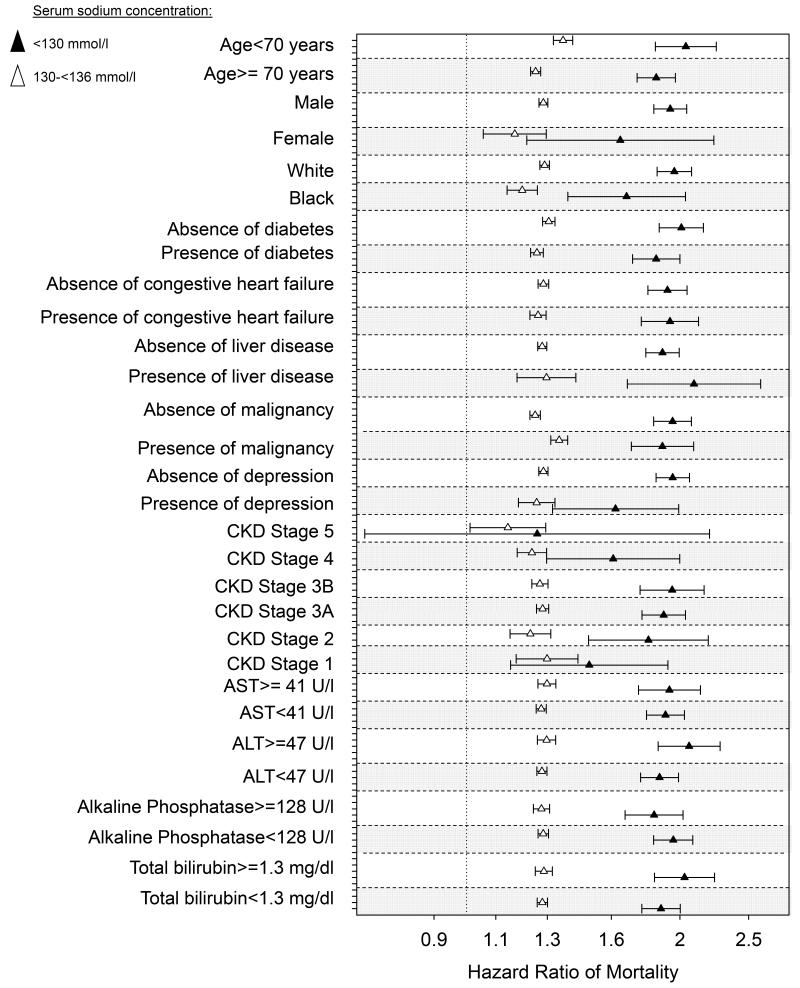
Methods and results: We examined the association of serum sodium concentration with all-cause mortality in a nationally representative cohort of 655 493 US veterans with non-dialysis-dependent chronic kidney disease (95 961 [15%] of them with congestive heart failure). Associations were examined in time-dependent Cox models with adjustment for potential confounders. During a median follow-up of 5.5 years, a total of 193 956 patients died (mortality rate, 62.5/1000 patient-years; 95% confidence interval, 62.2-62.8). The association of serum sodium level with mortality was U-shaped, with the lowest mortality seen in patients with sodium level of 140 mEq/L and with both lower and higher levels showing significant associations with increased mortality. Patients with serum sodium levels of <130, 130 to 135.9, 145.1 to 150, and ≥150 mEq/L compared with 136 to 145 mEq/L had multivariable-adjusted mortality hazard ratios (95% confidence interval) of 1.93 (1.83-2.03), 1.28 (1.26-1.30), 1.33 (1.28-1.38), and 1.56 (1.33-1.83) (P<0.001 for all). The associations remained consistent in subgroups of patients with and without congestive heart failure.
Conclusions: Both lower and higher serum sodium levels are independently associated with higher mortality in patients with non-dialysis-dependent chronic kidney disease, irrespective of the presence or absence of congestive heart failure.
Figures

References
-
- Upadhyay A, Jaber BL, Madias NE. Incidence and prevalence of hyponatremia. Am J Med. 2006;119:S30–S35. - PubMed
-
- Upadhyay A, Jaber BL, Madias NE. Epidemiology of hyponatremia. Semin Nephrol. 2009;29:227–238. - PubMed
-
- Anderson RJ, Chung HM, Kluge R, Schrier RW. Hyponatremia: a prospective analysis of its epidemiology and the pathogenetic role of vasopressin. Ann Intern Med. 1985;102:164–168. - PubMed
-
- Borroni G, Maggi A, Sangiovanni A, Cazzaniga M, Salerno F. Clinical relevance of hyponatraemia for the hospital outcome of cirrhotic patients. Dig Liver Dis. 2000;32:605–610. - PubMed
-
- Chung HM, Kluge R, Schrier RW, Anderson RJ. Postoperative hyponatremia. A prospective study. Arch Intern Med. 1986;146:333–336. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
