

Motion-compensated estimation of delivered dose during external beam radiation therapy: implementation in Philips' Pinnacle(3) treatment planning system
- PMID: 22225314
- PMCID: PMC3261057
- DOI: 10.1118/1.3670374
Motion-compensated estimation of delivered dose during external beam radiation therapy: implementation in Philips' Pinnacle(3) treatment planning system
Abstract
Purpose: Recent research efforts investigating dose escalation techniques for three-dimensional conformal radiation therapy (3D CRT) and intensity modulated radiation therapy (IMRT) have demonstrated great benefit when high-dose hypofractionated treatment schemes are implemented. The use of these paradigms emphasizes the importance of smaller treatment margins to avoid high dose to surrounding normal tissue or organs at risk (OARs). However, tighter margins may lead to underdosage of the target due to the presence of organ motion. It is important to characterize organ motion and possibly account for it during treatment delivery. The need for real-time localization of dynamic targets has encouraged the use and development of more continuous motion monitoring systems such as kilo-voltage/fluoroscopic imaging, electromagnetic tracking, and optical monitoring systems.
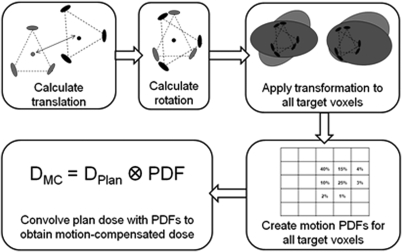
Methods: This paper presents the implementation of an algorithm to quantify translational and rotational interfractional and intrafractional prostate motion and compute the dosimetric effects of these motion patterns. The estimated delivered dose is compared with the static plan dose to evaluate the success of delivering the plan in the presence of prostate motion. The method is implemented on a commercial treatment planning system (Pinnacle(3), Philips Radiation Oncology Systems, Philips Healthcare) and is termed delivered dose investigational tool (DiDIT). The DiDIT implementation in Pinnacle(3) is validated by comparisons with previously published results. Finally, different workflows are discussed with respect to the potential use of this tool in clinical treatment planning.
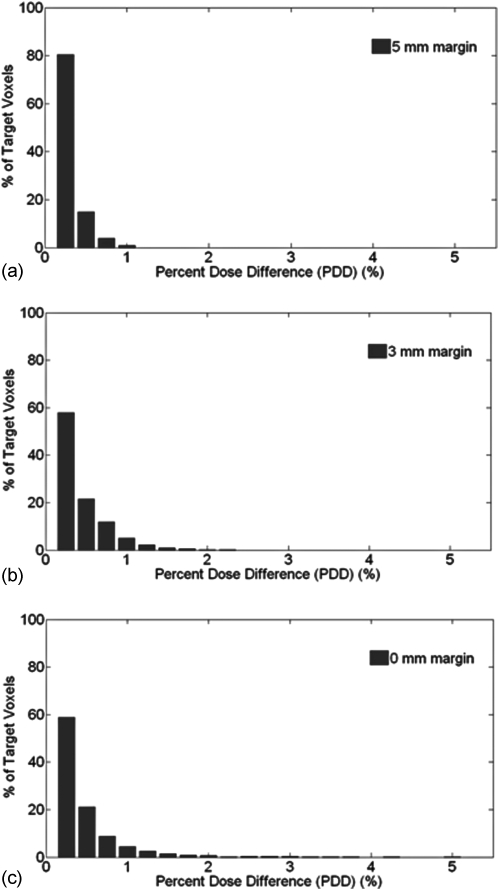
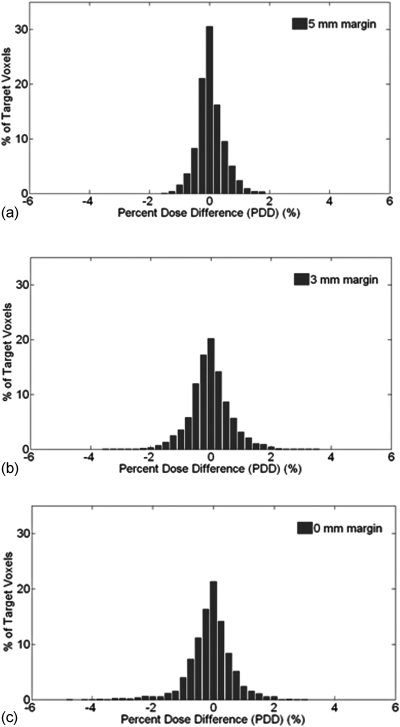
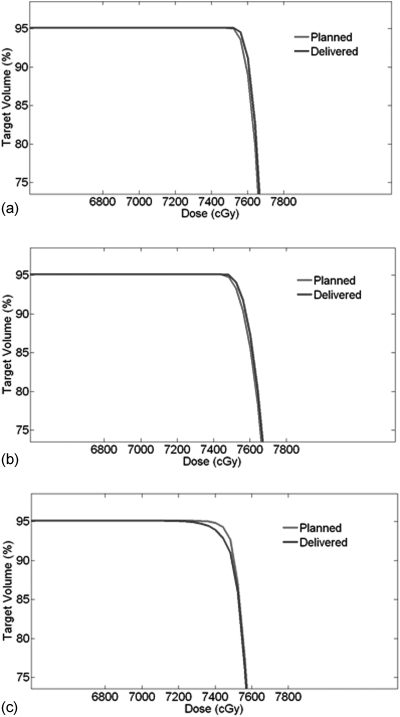
Results: The DiDIT dose estimation process took approximately 5-20 min (depending on the number of fractions analyzed) on a Pinnacle(3) 9.100 research version running on a Dell M90 system (Dell, Inc., Round Rock, TX, USA) equipped with an Intel Core 2 Duo processor (Intel Corporation, Santa Clara, CA, USA). The DiDIT implementation in Pinnacle(3) was found to be in agreement with previously published results, on the basis of the percent dose difference (PDD). This metric was also utilized to compare plan dose versus delivered dose, for prostate targets in three clinically acceptable treatment plans.
Conclusions: This paper presents results from the implementation of an algorithm on a commercially available treatment planning system that quantifies the dosimetric effects of interfractional and intrafractional motion in external beam radiation therapy (EBRT) of prostate cancer. The implementation of this algorithm within a commercial treatment planning system such as Pinnacle(3) enables easy deployment in the existing clinical workflow. The results of the PDD tests validate the implementation of the DiDIT algorithm in Pinnacle(3), in comparison with previously published results.
Figures
Similar articles
-
The use of spatial dose gradients and probability density function to evaluate the effect of internal organ motion for prostate IMRT treatment planning.Phys Med Biol. 2007 Mar 7;52(5):1469-84. doi: 10.1088/0031-9155/52/5/016. Epub 2007 Feb 12. Phys Med Biol. 2007. PMID: 17301465
-
Determination of action thresholds for electromagnetic tracking system-guided hypofractionated prostate radiotherapy using volumetric modulated arc therapy.Med Phys. 2011 Jul;38(7):4001-8. doi: 10.1118/1.3596776. Med Phys. 2011. PMID: 21858997 Free PMC article.
-
Evaluations of an adaptive planning technique incorporating dose feedback in image-guided radiotherapy of prostate cancer.Med Phys. 2011 Dec;38(12):6362-70. doi: 10.1118/1.3658567. Med Phys. 2011. PMID: 22149819 Free PMC article.
-
Intensity-modulated radiotherapy: current status and issues of interest.Int J Radiat Oncol Biol Phys. 2001 Nov 15;51(4):880-914. doi: 10.1016/s0360-3016(01)01749-7. Int J Radiat Oncol Biol Phys. 2001. PMID: 11704310 Review.
-
Image-guided radiotherapy: a new dimension in radiation oncology.Dtsch Arztebl Int. 2011 Apr;108(16):274-80. doi: 10.3238/arztebl.2011.0274. Epub 2011 Apr 22. Dtsch Arztebl Int. 2011. PMID: 21603562 Free PMC article. Review.
Cited by
-
Adaptive radiation therapy for postprostatectomy patients using real-time electromagnetic target motion tracking during external beam radiation therapy.Int J Radiat Oncol Biol Phys. 2013 Mar 15;85(4):1038-44. doi: 10.1016/j.ijrobp.2012.08.001. Epub 2012 Sep 25. Int J Radiat Oncol Biol Phys. 2013. PMID: 23021439 Free PMC article.
-
Effects on Periocular Tissues after Proton Beam Radiation Therapy for Intraocular Tumors.J Korean Med Sci. 2018 Apr 16;33(16):e120. doi: 10.3346/jkms.2018.33.e120. J Korean Med Sci. 2018. PMID: 29651818 Free PMC article.
-
A method of dose reconstruction for moving targets compatible with dynamic treatments.Med Phys. 2012 Oct;39(10):6237-46. doi: 10.1118/1.4754297. Med Phys. 2012. PMID: 23039659 Free PMC article.
References
-
- Sandler H. et al., “Reduction in patient-reported acute morbidity in prostate cancer patients treated with 81-Gy Intensity-modulated radiotherapy using reduced planning target volume margins and electromagnetic tracking: assessing the impact of margin reduction study,” Urology 75, 1004–1008 (2010).10.1016/j.urology.2009.10.072 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
