

Blood lipid levels, lipid-lowering medications, and the incidence of atrial fibrillation: the atherosclerosis risk in communities study
- PMID: 22227953
- PMCID: PMC3290134
- DOI: 10.1161/CIRCEP.111.966804
Blood lipid levels, lipid-lowering medications, and the incidence of atrial fibrillation: the atherosclerosis risk in communities study
Abstract
Background: Several cardiovascular risk factors have been associated with the risk of atrial fibrillation (AF). Limited and inconsistent evidence exists on the association of blood lipid levels and lipid-lowering medication use with AF risk.
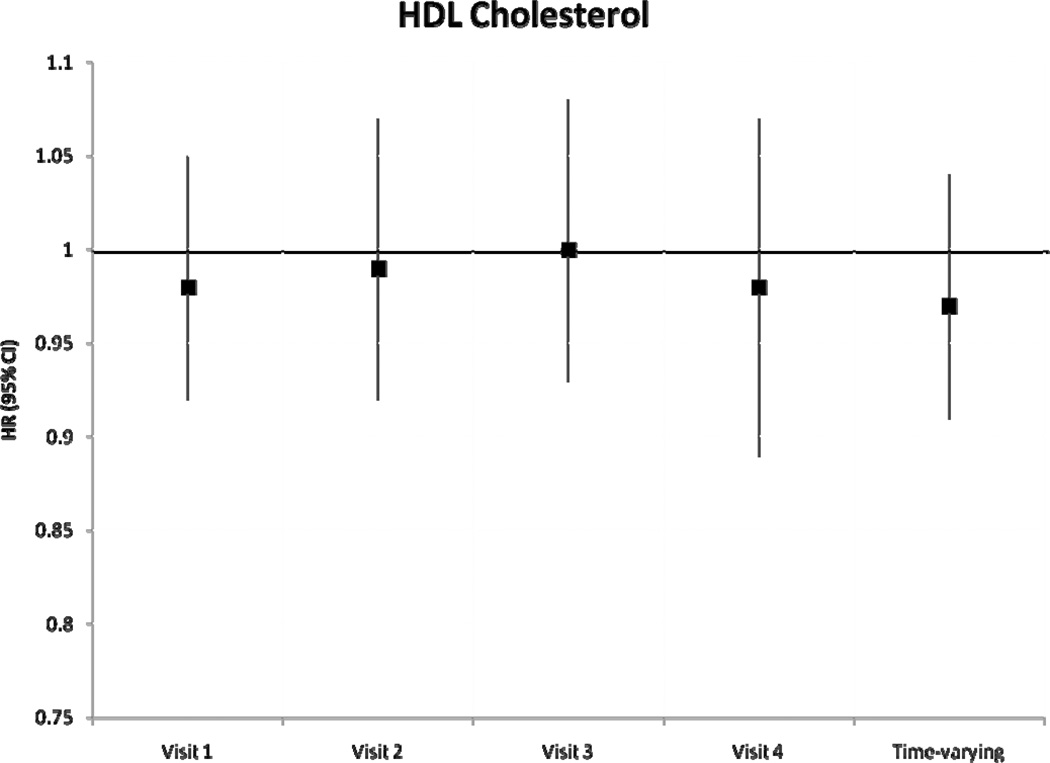
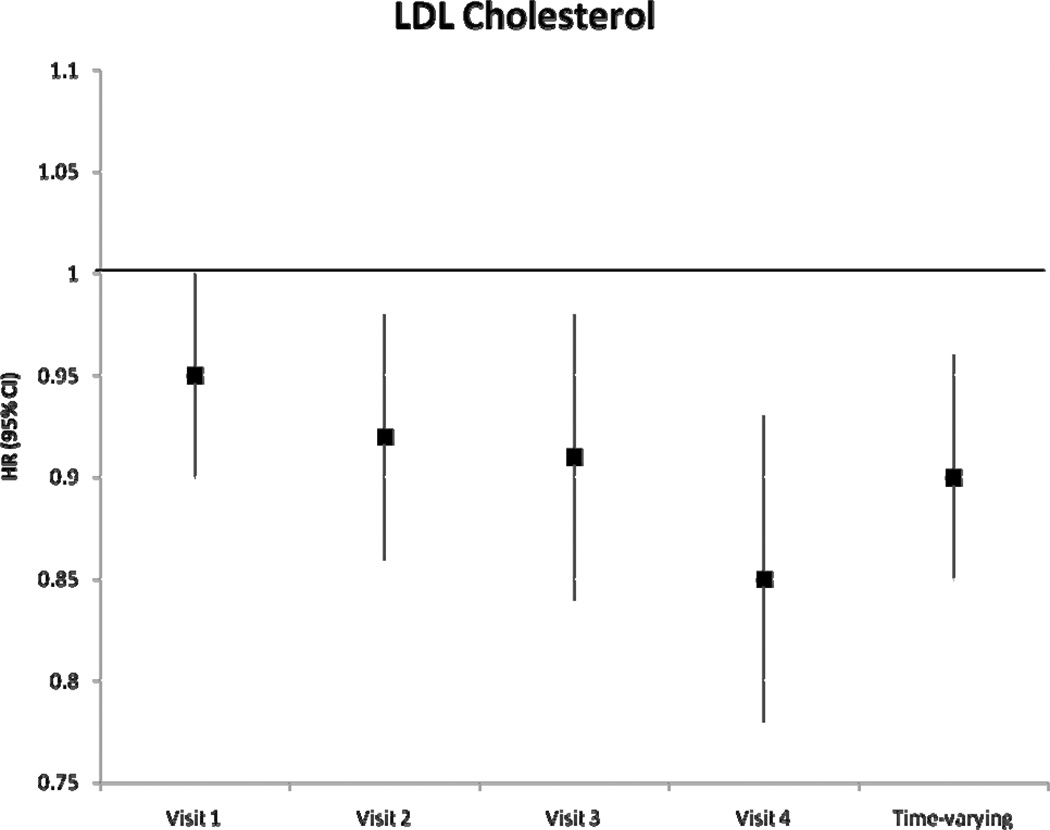
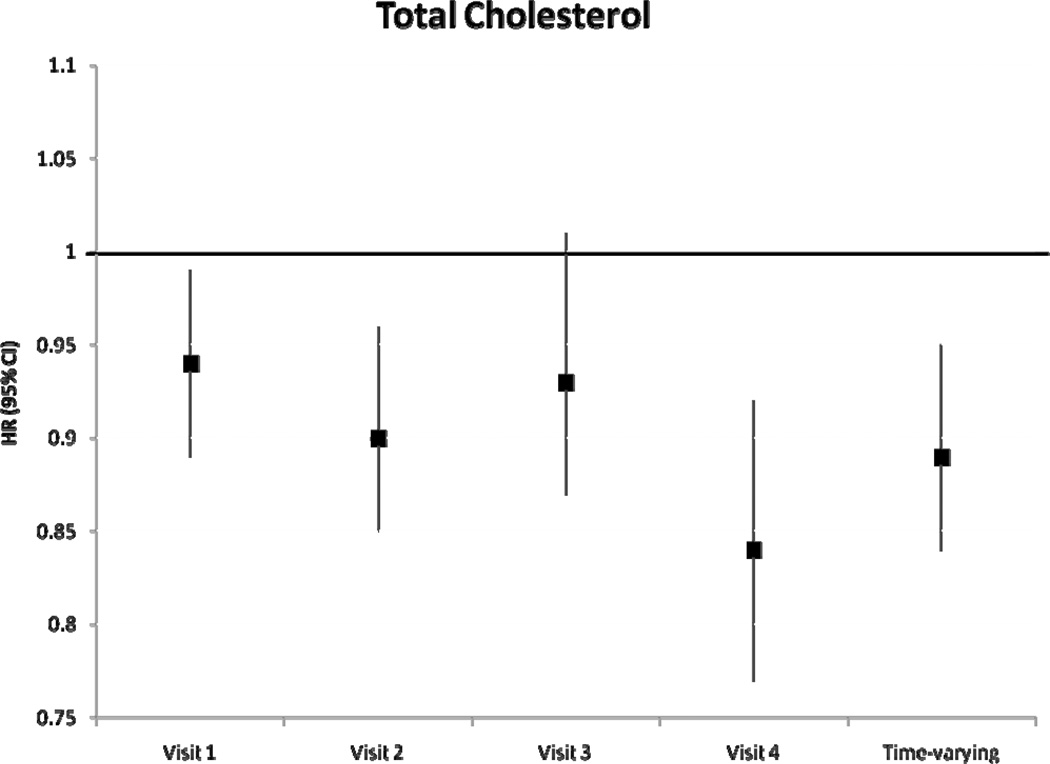
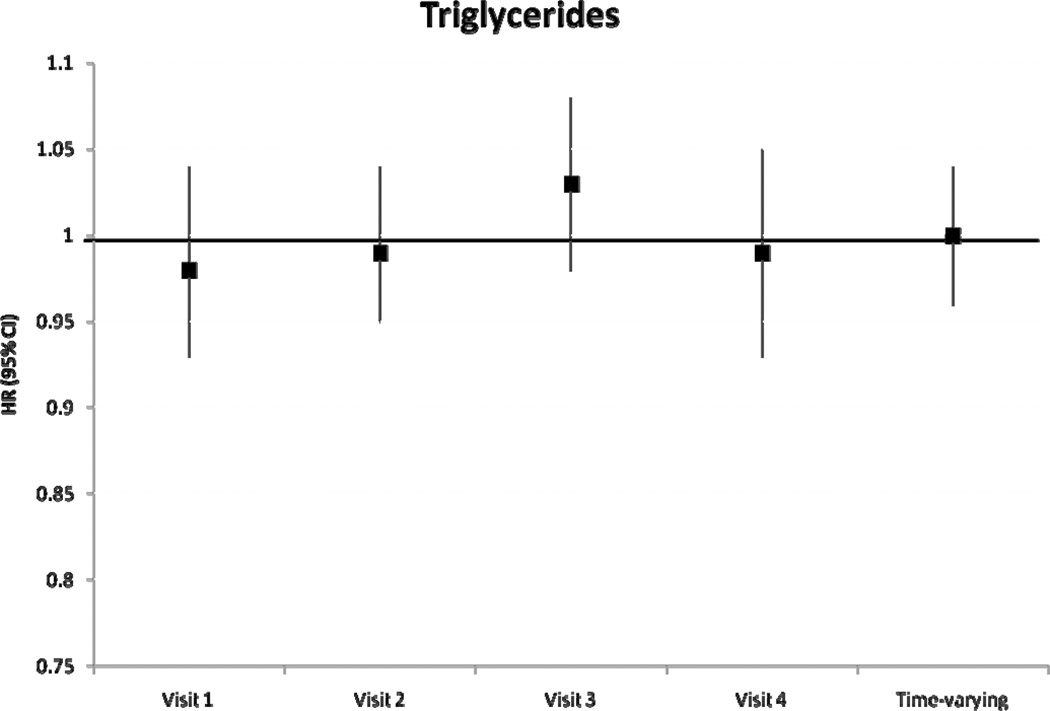
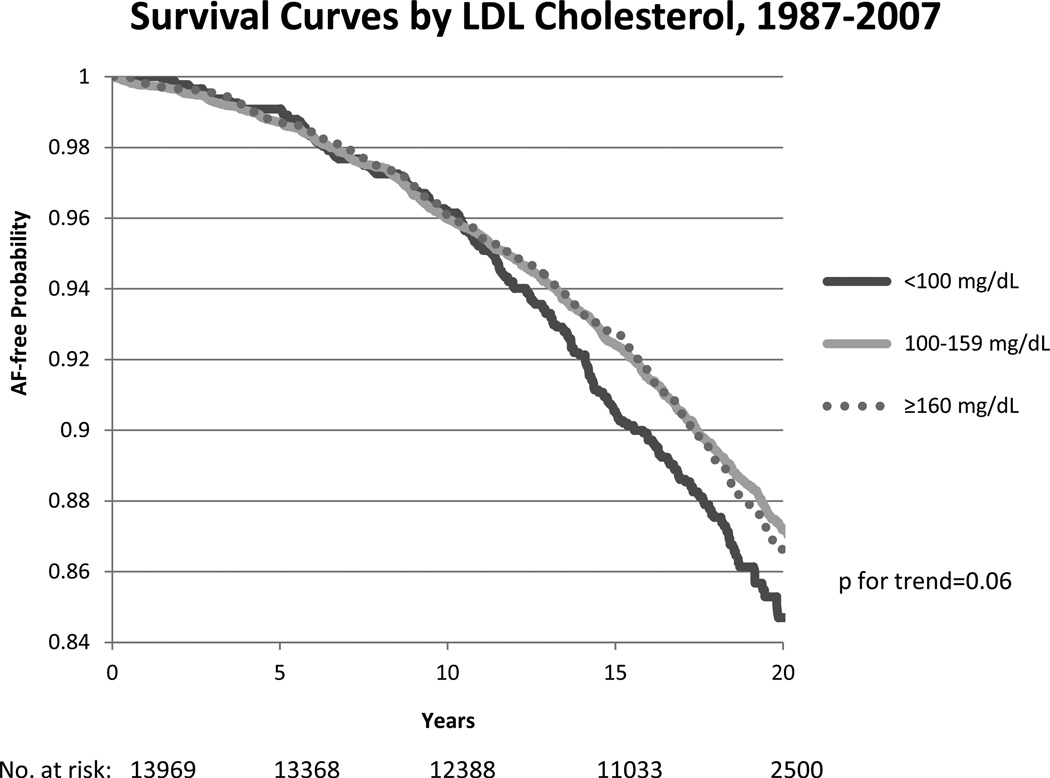
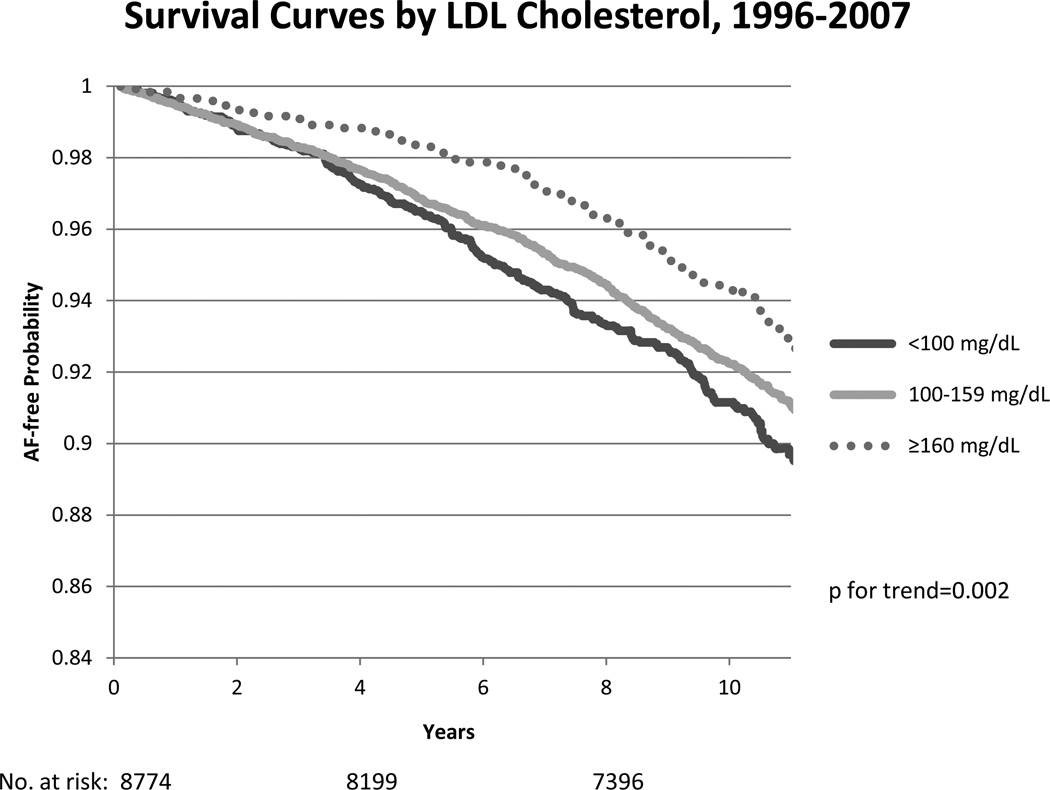
Methods and results: We analyzed 13 969 participants (25% African American, 45% men) free of AF at baseline from the Atherosclerosis Risk in Communities study. Fasting high-density lipoprotein cholesterol (HDLc), low-density lipoprotein cholesterol (LDLc), triglycerides, and total cholesterol were measured at baseline (1987-1989) and each of 3 follow-up visits. The incidence of AF was ascertained through 2007. The association of the use of statins and other lipid-lowering medications with AF was estimated in 13 044 Atherosclerosis Risk in Communities participants attending visit 2 (1990-1992), adjusting for covariates from the previous visit. During a median follow-up of 18.7 years, there were 1433 incident AF cases. Multivariable hazard ratios (HRs) and 95% CIs of AF associated with a 1-SD increase in lipid levels were as follows: HDLc, 0.97 (0.91-1.04); LDLc, 0.90 (0.85-0.96); total cholesterol, 0.89 (0.84-0.95); and triglycerides, 1.00 (0.96-1.04). Participants taking lipid-lowering medications had an adjusted HR (95% CI) of AF of 0.96 (0.82-1.13) compared with those not taking medications, whereas those taking statins had an adjusted HR of 0.91 (0.66-1.25) compared with those taking other lipid-lowering medications.
Conclusions: Higher levels of LDLc and total cholesterol were associated with a lower incidence of AF. However, HDLc and triglycerides were not independently associated with AF incidence. No association was found between the use of lipid-lowering medications and incident AF.
Conflict of interest statement
Figures
Comment in
-
Letter by Watanabe and Aizawa regarding article, "Blood lipid levels, lipid-lowering medications, and the incidence of atrial fibrillation: the Atherosclerosis Risk in Communities (ARIC) Study".Circ Arrhythm Electrophysiol. 2012 Jun 1;5(3):e80; author reply e81. doi: 10.1161/CIRCEP.112.971051. Circ Arrhythm Electrophysiol. 2012. PMID: 22715246 No abstract available.
References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA. 1994;271:840–844. - PubMed
-
- Sanoski CA. Prevalence, pathogenesis, and impact of atrial fibrillation. Am J Health Syst Pharm. 2010;67:S11–S16. - PubMed
-
- Wang TJ, Parise H, Levy D, D'Agostino RBS, Wolf PA, Vasan RS, Benjamin EJ. Obesity and the risk of new-onset atrial fibrillation. JAMA. 2004;292:2471–2477. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-HC55021/HC/NHLBI NIH HHS/United States
- 09SDG2280087/PHS HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- N01-HC55015/HC/NHLBI NIH HHS/United States
- N01 HC055018/HC/NHLBI NIH HHS/United States
- RC1 HL099452/HL/NHLBI NIH HHS/United States
- N01-HC55022/HC/NHLBI NIH HHS/United States
- N01-HC55019/HC/NHLBI NIH HHS/United States
- RC1-HL099452/HL/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01-HC55016/HC/NHLBI NIH HHS/United States
- N01 HC055016/HC/NHLBI NIH HHS/United States
- N01-HC55020/HC/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- N01 HC055019/HC/NHLBI NIH HHS/United States
- N01-HC55018/HC/NHLBI NIH HHS/United States
- N01 HC055015/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
