

Monocyte maturation, HIV susceptibility, and transmigration across the blood brain barrier are critical in HIV neuropathogenesis
- PMID: 22227964
- PMCID: PMC3289493
- DOI: 10.1189/jlb.0811394
Monocyte maturation, HIV susceptibility, and transmigration across the blood brain barrier are critical in HIV neuropathogenesis
Abstract
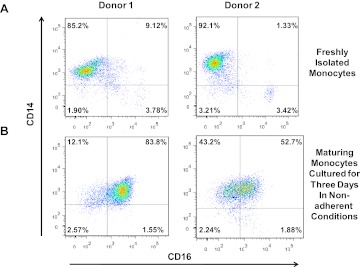
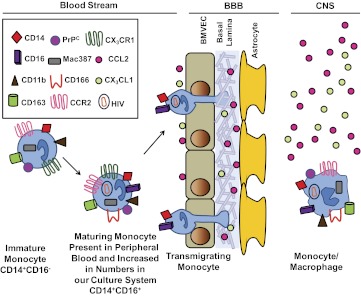
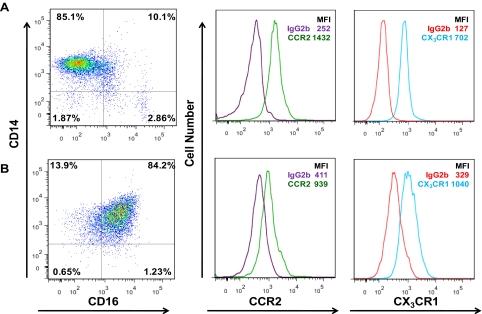
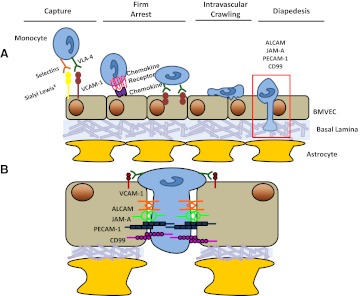
HIV continues to be a global health crisis with more than 34 million people infected worldwide (UNAIDS: Report on the Global AIDS Epidemic 2010, Geneva, World Health Organization). HIV enters the CNS within 2 weeks of infection and establishes a spectrum of HAND in a large percentage of infected individuals. These neurologic deficits greatly impact the quality of life of those infected with HIV. The establishment of HAND is largely attributed to monocyte transmigration, particularly that of a mature CD14(+)CD16(+) monocyte population, which is more susceptible to HIV infection, across the BBB into the CNS parenchyma in response to chemotactic signals. To enter the CNS, junctional proteins on the monocytes must participate in homo- and heterotypic interactions with those present on BMVECs of the BBB as they transmigrate across the barrier. This transmigration is responsible for bringing virus into the brain and establishing chronic neuroinflammation. While there is baseline trafficking of monocytes into the CNS, the increased chemotactic signals present during HIV infection of the brain promote exuberant monocyte transmigration into the CNS. This review will discuss the mechanisms of monocyte differentiation/maturation, HIV infectivity, and transmigration into the CNS parenchyma that contribute to the establishment of cognitive impairment in HIV-infected individuals. It will focus on markers of monocyte subpopulations, how differentiation/maturation alters HIV infectivity, and the mechanisms that promote their increased transmigration across the BBB into the CNS.
Figures

References
-
- Graham N. M. H., Zeger S. L., Park L. P., Vermund S. H., Detels R., Rinaldo C. R., Phair J. P. (1992) The effects on survival of early treatment of human immunodeficiency virus infection. N. Engl. J. Med. 326, 1037–1042 - PubMed
-
- Hammer S. M., Squires K. E., Hughes M. D., Grimes J. M., Demeter L. M., Currier J. S., Eron J. J., Jr., Feinberg J. E., Balfour H. H., Jr., Deyton L. R., Chodakewitz J. A., Fischl M. A. (1997) A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. N. Engl. J. Med. 337, 725–733 - PubMed
-
- Li T. S., Tubiana R., Katlama C., Calvez V., Mohand H. A., Autran B. (1998) Long-lasting recovery in CD4 T-cell function and viral-load reduction after highly active antiretroviral therapy in advanced HIV-1 disease. Lancet 351, 1682–1686 - PubMed
-
- Hunt P. W., Deeks S. G., Rodriguez B., Valdez H., Shade S. B., Abrams D. I., Kitahata M. M., Krone M., Neilands T. B., Brand R. J., Lederman M. M., Martin J. N. (2003) Continued CD4 cell count increases in HIV-infected adults experiencing 4 years of viral suppression on antiretroviral therapy. AIDS 17, 1907–1915 - PubMed
-
- Ances B., Ellis R. (2007) Dementia and neurocognitive disorders due to HIV-1 infection. Semin. Neurol. 27, 086–092 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
