

Beyond 30 days: does limiting the duration of surgical site infection follow-up limit detection?
- PMID: 22227993
- PMCID: PMC3608264
- DOI: 10.1086/663715
Beyond 30 days: does limiting the duration of surgical site infection follow-up limit detection?
Abstract
Concern over consistency and completeness of surgical site infection (SSI) surveillance has increased due to public reporting of hospital SSI rates and imminent non-payment rules for hospitals that do not meet national benchmarks. Already, hospitals no longer receive additional payment from the Centers for Medicare & Medicaid Services (CMS) for certain infections following coronary artery bypass graft (CABG) surgery, orthopedic procedures, and bariatric surgery.
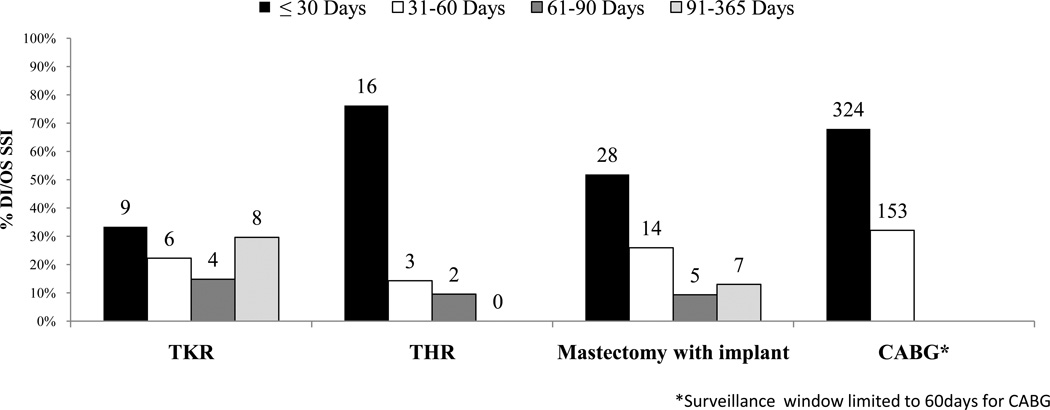
One major concern is incomplete and differential post-discharge surveillance. At present, substantial variation exists in how and whether hospitals identify SSI events after the hospitalization in which the surgery occurred. Parameters used for SSI surveillance such as the duration of the window of time that surveillance takes place following the surgical procedure can impact the completeness of surveillance data. Determination of the optimal surveillance time period involves balancing the potential increased case ascertainment associated with a longer follow-up period with the increased resources that would be required. Currently, the time window for identifying potentially preventable SSIs related to events at the time of surgery is not fully standardized. The Centers for Disease Control and Prevention (CDC) National Healthcare Surveillance Network (NHSN) requires a 365-day postoperative surveillance period for procedures involving implants and a 30-day period for non-implant procedures. In contrast, the National Surgical Quality Improvement Program (NSQIP) and the Society of Thoracic Surgeons (STS) systems employ 30-day post-operative surveillance regardless of implant. As consensus builds towards national quality measures for hospital-specific SSI rates, it will be important to assess the frequency of events beyond the 30-day post-surgical window that may quantify the value of various durations of surveillance, and ultimately inform the choice of specific outcome measures.
Conflict of interest statement
All authors report no conflicts of interest relevant to this article.
Figures
Comment in
-
How long is long enough? Determining the optimal surgical site infection surveillance period.Infect Control Hosp Epidemiol. 2012 Nov;33(11):1178-9. doi: 10.1086/668037. Infect Control Hosp Epidemiol. 2012. PMID: 23041824 No abstract available.
References
-
- Rosenthal MB. Nonpayment for performance? Medicare's new reimbursement rule. N Engl J Med. 2007 Oct 18;357(16):1573–1575. - PubMed
-
- Medicare program; changes to the hospital inpatient prospective payment systems and fiscal year 2008 rates. Fed Regist. 2007 Aug 22;72(162):47129–48175. - PubMed
-
- Horan TC, Andrus M, Dudeck M. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309–332. - PubMed
-
- Yokoe D. Multicenter Evaluation of Enhanced Methods for Surgical Site Infection Surveillance Following Total Hip and Total Knee Arthroplasty. Presented at the Fifth Decennial International Conference on Healthcare-Associated Infections; April 2010; Atlanta, GA.
-
- Bolon MK, Hooper D, Stevenson KB, et al. Improved surveillance for surgical site infections after orthopedic implantation procedures: extending applications for automated data. Clin Infect Dis. 2009;48:1223–1229. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials