

Immunochemotherapy with intensive consolidation for primary CNS lymphoma: a pilot study and prognostic assessment by diffusion-weighted MRI
- PMID: 22228634
- PMCID: PMC3288204
- DOI: 10.1158/1078-0432.CCR-11-0625
Immunochemotherapy with intensive consolidation for primary CNS lymphoma: a pilot study and prognostic assessment by diffusion-weighted MRI
Abstract
Purpose: We evaluated a novel therapy for primary central nervous system lymphoma (PCNSL) with induction immunochemotherapy with high-dose methotrexate, temozolomide, and rituximab (MT-R) followed by intensive consolidation with infusional etoposide and high-dose cytarabine (EA). In addition, we evaluated the prognostic value of the minimum apparent diffusion coefficient (ADC(min)) derived from diffusion-weighted MRI (DW-MRI) in patients treated with this regimen.
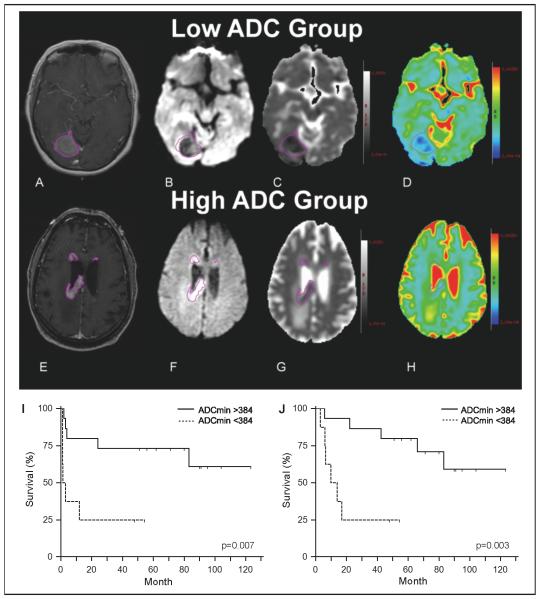
Experimental design: Thirty-one patients (median age, 61 years; median Karnofsky performance score, 60) received induction with methotrexate every 14 days for 8 planned cycles. Rituximab was administered the first 6 cycles and temozolomide administered on odd-numbered cycles. Patients with responsive or stable central nervous system (CNS) disease received EA consolidation. Pretreatment DW-MRI was used to calculate the ADC(min) of contrast-enhancing lesions.
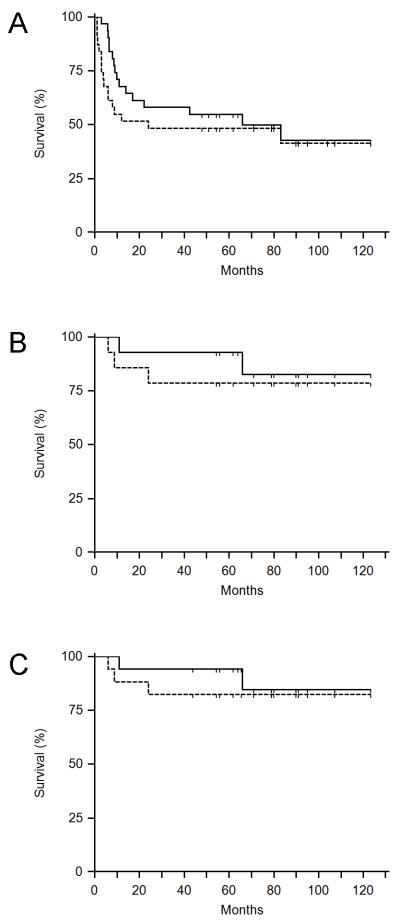
Results: The complete response rate for MT-R induction was 52%. At a median follow-up of 79 months, the 2-year progression-free and overall survival were 45% and 58%, respectively. For patients receiving EA consolidation, the 2-year progression-free and overall survival were 78% and 93%, respectively. EA consolidation was also effective in an additional 3 patients who presented with synchronous CNS and systemic lymphoma. Tumor ADC(min) less than 384 × 10(-6) mm(2)/s was significantly associated with shorter progression-free and overall survival.
Conclusions: MT-R induction was effective and well tolerated. MT-R followed by EA consolidation yielded progression-free and overall survival outcomes comparable to regimens with chemotherapy followed by whole-brain radiotherapy consolidation but without evidence of neurotoxicity. Tumor ADC(min) derived from DW-MRI provided better prognostic information for PCNSL patients treated with the MTR-EA regimen than established clinical risk scores.
©2012 AACR.
Figures
References
-
- Abrey LE, DeAngelis LM, Yahalom J. Long-term survival in primary CNS lymphoma. J Clin Oncol. 1998;16:859–63. - PubMed
-
- Shah GD, Yahalom J, Correa DD, Lai RK, Raizer JJ, Schiff D, LaRocca R, Grant B, DeAngelis LM, Abrey LE. Combined immunochemotherapy with reduced whole-brain radiotherapy for newly diagnosed primary CNS lymphoma. J Clin Oncol. 2007;25:4730–5. - PubMed
-
- Blay JY, Conroy T, Chevreau C, Thyss A, Quesnel N, Eghbali H, Bouabdallah R, Coiffier B, Wagner JP, Le Mevel A, Dramais-Marcel D, Baumelou E, Chauvin F, Biron P. High-dose methotrexate for the treatment of primary cerebral lymphomas: analysis of survival and late neurologic toxicity in a retrospective series. J Clin Oncol. 1998;16:864–71. - PubMed
-
- Fliessbach K, Helmstaedter C, Urbach H, Althaus A, Pels H, Linnebank M, Juergens A, Glasmacher A, Schmidt-Wolf IG, Klockgether T, Schlegel U. Neuropsychological outcome after chemotherapy for primary CNS lymphoma: a prospective study. Neurology. 2005;64:1184–8. - PubMed
-
- Batchelor T, Carson K, O’Neill A, Grossman SA, Alavi J, New P, Hochberg F, Priet R. Treatment of primary CNS lymphoma with methotrexate and deferred radiotherapy: a report of NABTT 96-07. J Clin Oncol. 2003;21:1044–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
