

Neuropathological alterations in Alzheimer disease
- PMID: 22229116
- PMCID: PMC3234452
- DOI: 10.1101/cshperspect.a006189
Neuropathological alterations in Alzheimer disease
Abstract
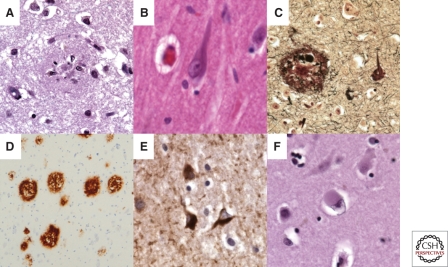
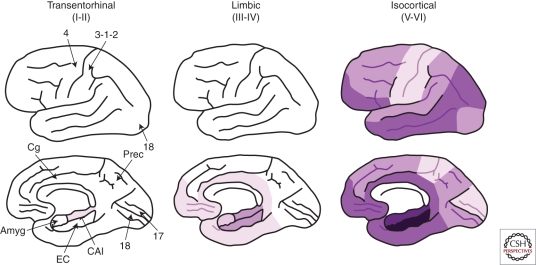
The neuropathological hallmarks of Alzheimer disease (AD) include "positive" lesions such as amyloid plaques and cerebral amyloid angiopathy, neurofibrillary tangles, and glial responses, and "negative" lesions such as neuronal and synaptic loss. Despite their inherently cross-sectional nature, postmortem studies have enabled the staging of the progression of both amyloid and tangle pathologies, and, consequently, the development of diagnostic criteria that are now used worldwide. In addition, clinicopathological correlation studies have been crucial to generate hypotheses about the pathophysiology of the disease, by establishing that there is a continuum between "normal" aging and AD dementia, and that the amyloid plaque build-up occurs primarily before the onset of cognitive deficits, while neurofibrillary tangles, neuron loss, and particularly synaptic loss, parallel the progression of cognitive decline. Importantly, these cross-sectional neuropathological data have been largely validated by longitudinal in vivo studies using modern imaging biomarkers such as amyloid PET and volumetric MRI.
Figures

References
-
- Aarsland D, Ballard CG, Halliday G 2004. Are Parkinson’s disease with dementia and dementia with Lewy bodies the same entity? J Geriatr Psychiatry Neurol 17: 137–145 - PubMed
-
- Arnold SE, Hyman BT, Flory J, Damasio AR, Van Hoesen GW 1991. The topographical and neuroanatomical distribution of neurofibrillary tangles and neuritic plaques in the cerebral cortex of patients with Alzheimer’s disease. Cereb Cortex 1: 103–116 - PubMed
-
- Arriagada PV, Growdon JH, Hedley-Whyte ET, Hyman BT 1992a. Neurofibrillary tangles but not senile plaques parallel duration and severity of Alzheimer’s disease. Neurology 42: 631–639 - PubMed
-
- Arriagada PV, Marzloff K, Hyman BT 1992b. Distribution of Alzheimer-type pathologic changes in non-demented elderly individuals matches the pattern in Alzheimer’s disease. Neurology 42: 1681–1688 - PubMed
Publication types
MeSH terms
Grants and funding
- P50AG05134/AG/NIA NIH HHS/United States
- NS057096/NS/NINDS NIH HHS/United States
- AG10435/AG/NIA NIH HHS/United States
- P50 AG005131/AG/NIA NIH HHS/United States
- U19 AG010483/AG/NIA NIH HHS/United States
- R01 AG008487/AG/NIA NIH HHS/United States
- AG18840/AG/NIA NIH HHS/United States
- P01 AG022074/AG/NIA NIH HHS/United States
- AG22074/AG/NIA NIH HHS/United States
- P30 NS057096/NS/NINDS NIH HHS/United States
- P50 AG005134/AG/NIA NIH HHS/United States
- R37 AG018440/AG/NIA NIH HHS/United States
- P01 AG010435/AG/NIA NIH HHS/United States
- AG08487/AG/NIA NIH HHS/United States
- AG5131/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical