

Pre-injury polypharmacy as a predictor of outcomes in trauma patients
- PMID: 22229132
- PMCID: PMC3249840
- DOI: 10.4103/2229-5151.84793
Pre-injury polypharmacy as a predictor of outcomes in trauma patients
Abstract
Background: One of the hallmarks of modern medicine is the improving management of chronic health conditions. Long-term control of chronic disease entails increasing utilization of multiple medications and resultant polypharmacy. The goal of this study is to improve our understanding of the impact of polypharmacy on outcomes in trauma patients 45 years and older.
Materials and methods: Patients of age ≥45 years were identified from a Level I trauma center institutional registry. Detailed review of patient records included the following variables: Home medications, comorbid conditions, injury severity score (ISS), Glasgow coma scale (GCS), morbidity, mortality, hospital length of stay (LOS), intensive care unit (ICU) LOS, functional outcome measures (FOM), and discharge destination. Polypharmacy was defined by the number of medications: 0-4 (minor), 5-9 (major), or ≥10 (severe). Age- and ISS-adjusted analysis of variance and multivariate analyses were performed for these groups. Comorbidity-polypharmacy score (CPS) was defined as the number of pre-admission medications plus comorbidities. Statistical significance was set at alpha = 0.05.
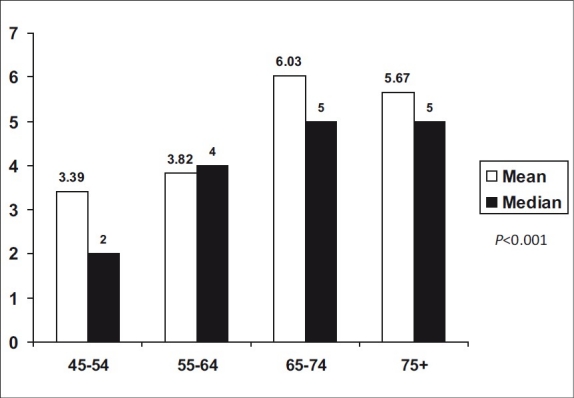
Results: A total of 323 patients were examined (mean age 62.3 years, 56.1% males, median ISS 9). Study patients were using an average of 4.74 pre-injury medications, with the number of medications per patient increasing from 3.39 for the 45-54 years age group to 5.68 for the 75+ year age group. Age- and ISS-adjusted mortality was similar in the three polypharmacy groups. In multivariate analysis only age and ISS were independently predictive of mortality. Increasing polypharmacy was associated with more comorbidities, lower arrival GCS, more complications, and lower FOM scores for self-feeding and expression-communication. In addition, hospital and ICU LOS were longer for patients with severe polypharmacy. Multivariate analysis shows age, female gender, total number of injuries, number of complications, and CPS are independently associated with discharge to a facility (all, P < 0.02).
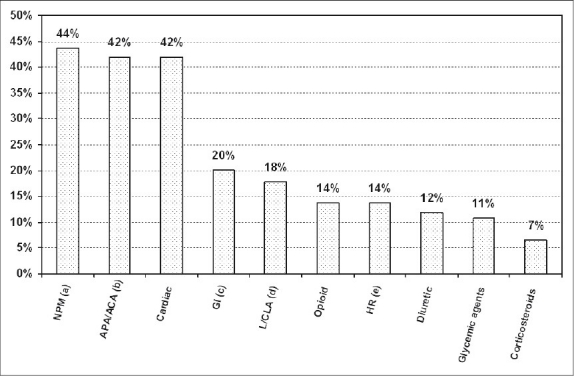
Conclusion: Over 40% of trauma patients 45 years and older were receiving 5 or more medications at the time of their injury. Although these patients do not appear to have higher mortality, they are at increased risk for complications, lower functional outcomes, and longer hospital and intensive care stays. CPS may be useful when quantifying the severity of associated comorbid conditions in the context of traumatic injury and warrants further investigation.
Keywords: Comorbid conditions; outcome prediction; polypharmacy; trauma outcomes.
Conflict of interest statement
Figures
References
-
- Stawicki SP, Gerlach AT. Polypharmacy and medication errors: Stop, Listen, Look, and Analyze. OPUS 12. Scientist. 2009;3:6–10.
-
- Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. Improving chronic illness care: Translating evidence into action. Health Aff (Millwood) 2001;20:64–78. - PubMed
-
- Montamat SC, Cusack B. Overcoming problems with polypharmacy and drug misuse in the elderly. Clin Geriatr Med. 1992;8:143–58. - PubMed
