

Randomized controlled trial of a lay-facilitated angina management programme
- PMID: 22229483
- PMCID: PMC3491702
- DOI: 10.1111/j.1365-2648.2011.05920.x
Randomized controlled trial of a lay-facilitated angina management programme
Abstract
Aims: This article reports a randomized controlled trial of lay-facilitated angina management (registered trial acronym: LAMP).
Background: Previously, a nurse-facilitated angina programme was shown to reduce angina while increasing physical activity, however most people with angina do not receive a cardiac rehabilitation or self-management programme. Lay people are increasingly being trained to facilitate self-management programmes.
Design: A randomized controlled trial comparing a lay-facilitated angina management programme with routine care from an angina nurse specialist.
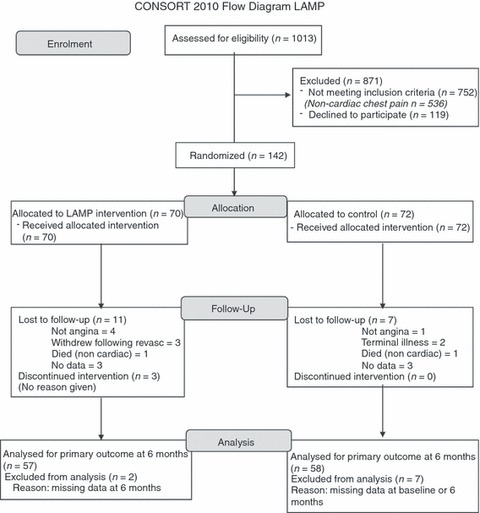
Methods: Participants with new stable angina were randomized to the angina management programme (intervention: 70 participants) or advice from an angina nurse specialist (control: 72 participants). Primary outcome was angina frequency at 6 months; secondary outcomes at 3 and 6 months included: risk factors, physical functioning, anxiety, depression, angina misconceptions and cost utility. Follow-up was complete in March 2009. Analysis was by intention-to-treat; blind to group allocation.
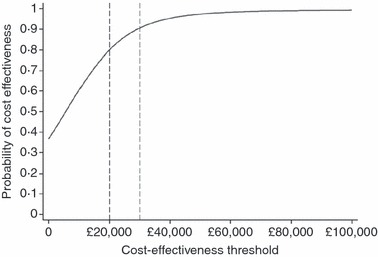
Results: There was no important difference in angina frequency at 6 months. Secondary outcomes, assessed by either linear or logistic regression models, demonstrated important differences favouring the intervention group, at 3 months for: Anxiety, angina misconceptions and for exercise report; and at 6 months for: anxiety; depression; and angina misconceptions. The intervention was considered cost-effective.
Conclusion: The angina management programme produced some superior benefits when compared to advice from a specialist nurse.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- Bakhai A, Ferrieres J, Iñiguez A, Schmitt C, Sartral M, Belger M, Zeymer U. International data on supportive therapies at 1 year in acute coronary syndrome patients undergoing PCI: results from the APTOR study. European Journal of Cardiovascular Prevention & Rehabilitation. 2011;18(3):518–525. - PubMed
-
- Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JM, Franklin B, Sanderson B, Southard D. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update. Circulation. 2007;115(20):2675–2682. - PubMed
-
- British Association for Cardiac Rehabilitation. Standards and Core Components for Cardiac Rehabilitation. London: BACR; 2007.
-
- Brook R. Euroqol: the current state of play. Health Policy. 1996;37:53–72. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
