

The cardioprotective association of average alcohol consumption and ischaemic heart disease: a systematic review and meta-analysis
- PMID: 22229788
- PMCID: PMC3348338
- DOI: 10.1111/j.1360-0443.2012.03780.x
The cardioprotective association of average alcohol consumption and ischaemic heart disease: a systematic review and meta-analysis
Abstract
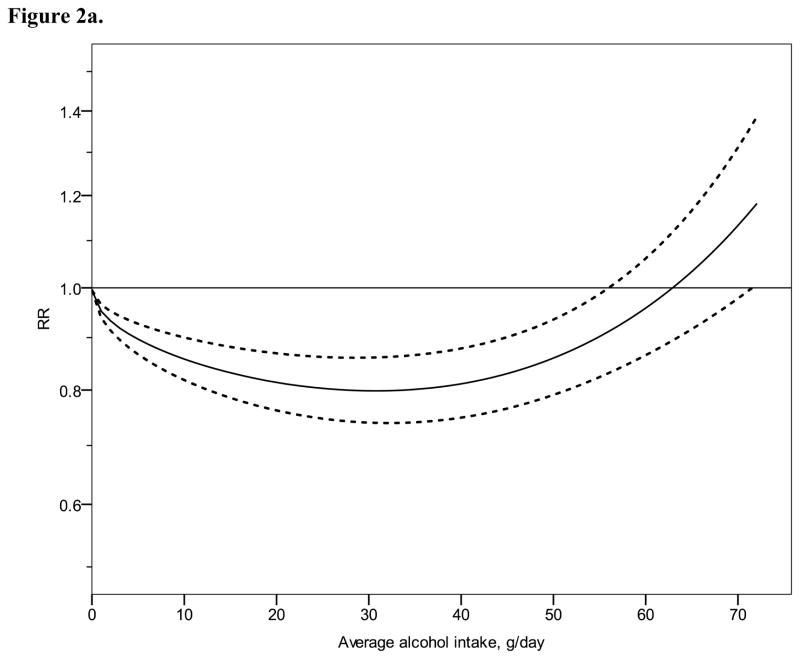
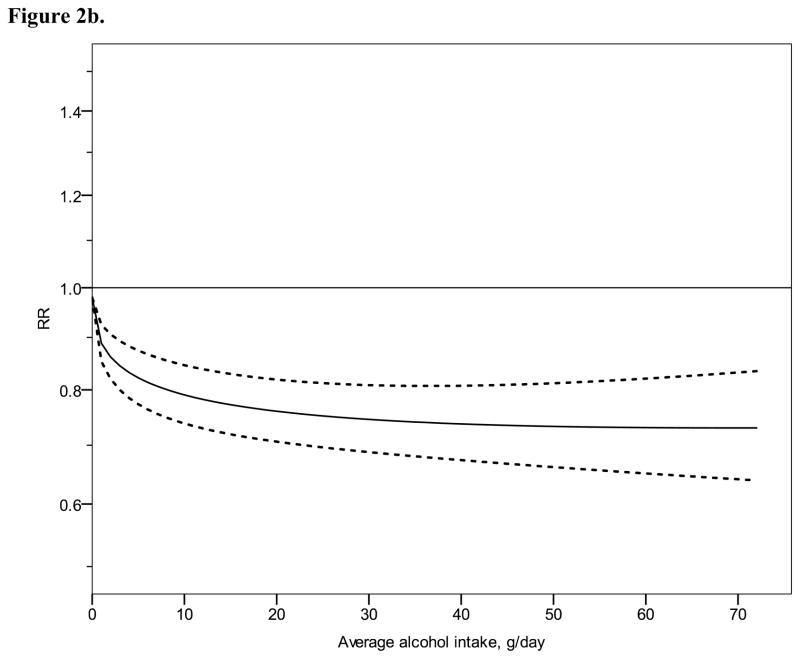
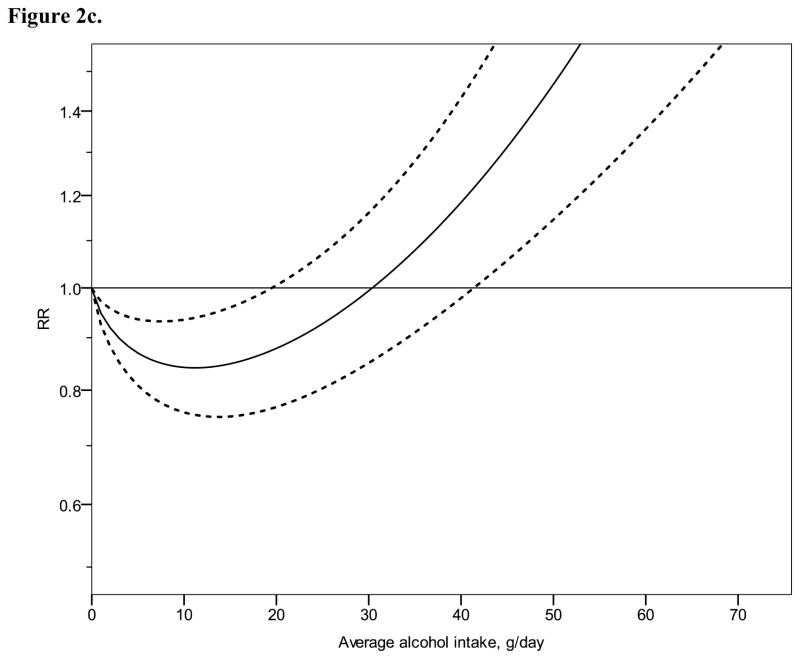
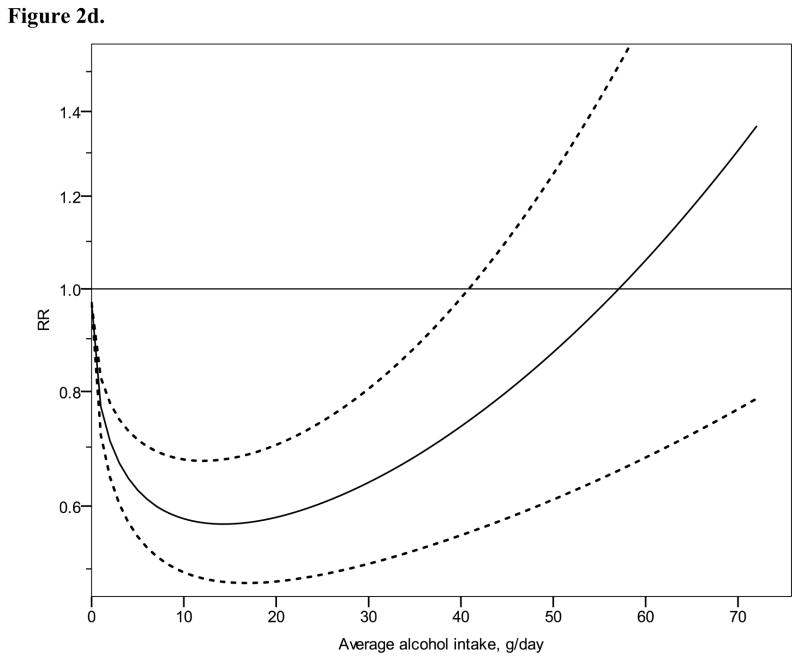
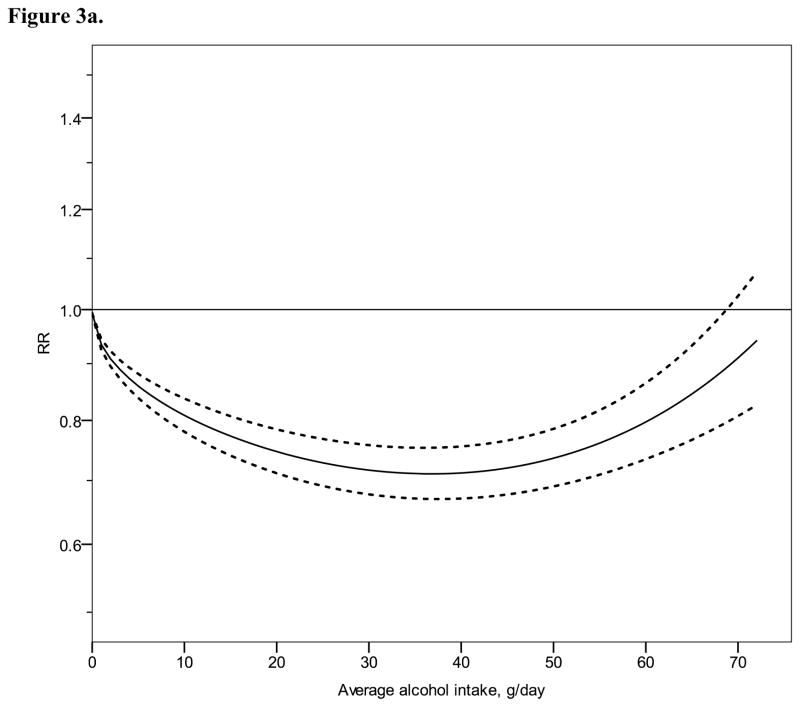
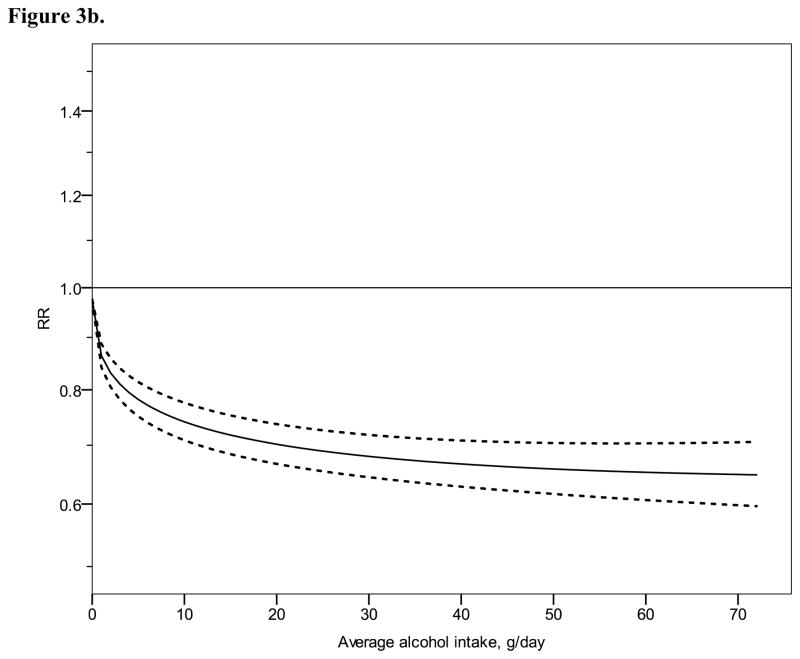
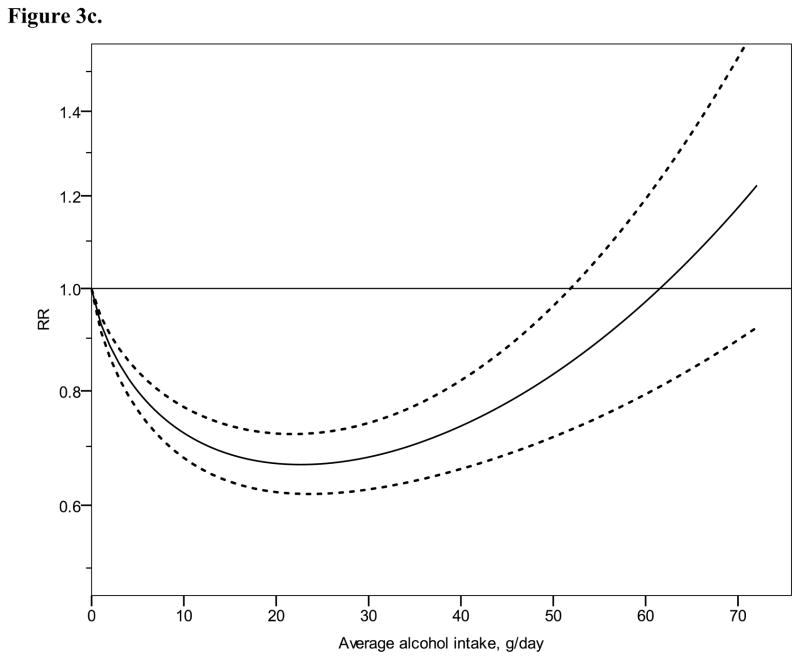
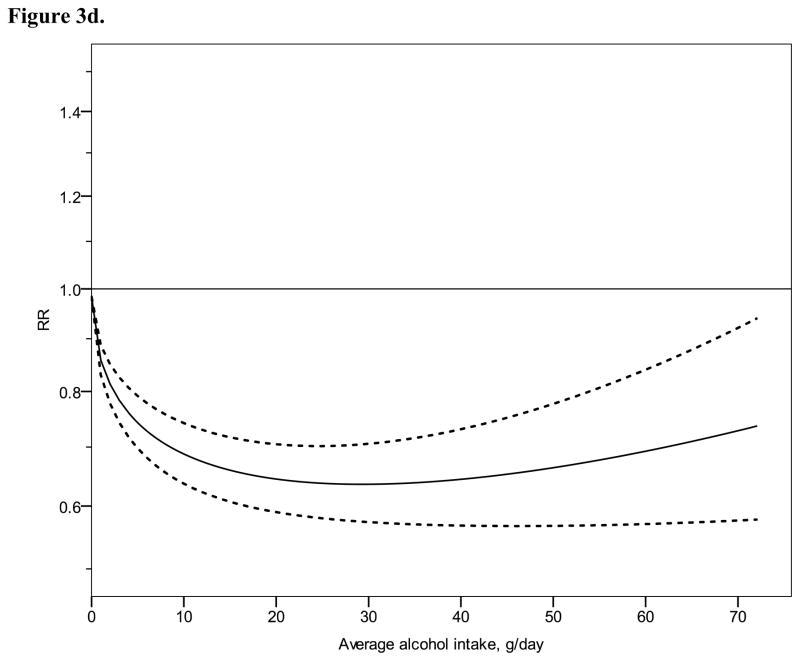
Aims: Most, but not all, epidemiological studies suggest a cardioprotective association for low to moderate average alcohol consumption. The objective was to quantify the dose-response relationship between average alcohol consumption and ischaemic heart disease (IHD) stratified by sex and IHD end-point (mortality versus morbidity).
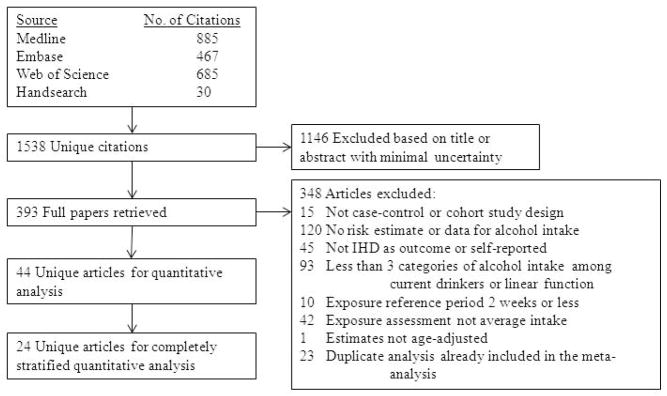
Methods: A systematic search of published studies using electronic databases (1980-2010) identified 44 observational studies (case-control or cohort) reporting a relative risk measure for average alcohol intake in relation to IHD risk. Generalized least-squares trend models were used to derive the best-fitting dose-response curves in stratified continuous meta-analyses. Categorical meta-analyses were used to verify uncertainty for low to moderate levels of consumption in comparison to long-term abstainers.
Results: The analyses used 38,627 IHD events (mortality or morbidity) among 957,684 participants. Differential risk curves were found by sex and end-point. Although some form of a cardioprotective association was confirmed in all strata, substantial heterogeneity across studies remained unexplained and confidence intervals were relatively wide, in particular for average consumption of one to two drinks/day.
Conclusions: A cardioprotective association between alcohol use and ischaemic heart disease cannot be assumed for all drinkers, even at low levels of intake. More evidence on the overall benefit-risk ratio of average alcohol consumption in relation to ischaemic heart disease and other diseases is needed in order to inform the general public or physicians about safe or low-risk drinking levels.
© 2012 The Authors, Addiction © 2012 Society for the Study of Addiction.
Conflict of interest statement
Declarations of interest:
All other authors have no interests to declare.
Figures
Comment in
-
Commentary on Roerecke & Rehm (2012): The state of the science on moderate drinking and health--a case of heterogeneity in and heterogeneity out?Addiction. 2012 Jul;107(7):1261-2. doi: 10.1111/j.1360-0443.2012.03866.x. Addiction. 2012. PMID: 22672375 No abstract available.
-
On the evidence of a cardioprotective effect of alcohol consumption.Addiction. 2013 Feb;108(2):429-31. doi: 10.1111/add.12076. Addiction. 2013. PMID: 23331886 No abstract available.
References
-
- Mukamal KJ, Phillips RS, Mittleman MA. Beliefs, motivations, and opinions about moderate drinking: A cross-sectional survey. Fam Med. 2008;40:188–195. - PubMed
-
- Corrao G, Rubbiati L, Bagnardi V, Zambon A, Poikolainen K. Alcohol and coronary heart disease: a meta-analysis. Addiction. 2000;95:1505–1523. - PubMed
-
- Costanzo S, Di Castelnuovo A, Donati MB, Iacoviello L, de Gaetano G. Alcohol consumption and mortality in patients with cardiovascular disease: a meta-analysis. J Am Coll Cardiol. 2010;55:1339–1347. - PubMed
-
- Maclure M. Demonstration of deductive metaanalysis - ethanol intake and risk of myocardial infarction. Epidemiol Rev. 1993;15:328–351. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
