

Online tool to guide decisions for BRCA1/2 mutation carriers
- PMID: 22231042
- PMCID: PMC3295552
- DOI: 10.1200/JCO.2011.38.6060
Online tool to guide decisions for BRCA1/2 mutation carriers
Abstract
Purpose: Women with BRCA1 or BRCA2 (BRCA1/2) mutations must choose between prophylactic surgeries and screening to manage their high risks of breast and ovarian cancer, comparing options in terms of cancer incidence, survival, and quality of life. A clinical decision tool could guide these complex choices.
Methods: We built a Monte Carlo model for BRCA1/2 mutation carriers, simulating breast screening with annual mammography plus magnetic resonance imaging (MRI) from ages 25 to 69 years and prophylactic mastectomy (PM) and/or prophylactic oophorectomy (PO) at various ages. Modeled outcomes were cancer incidence, tumor features that shape treatment recommendations, overall survival, and cause-specific mortality. We adapted the model into an online tool to support shared decision making.
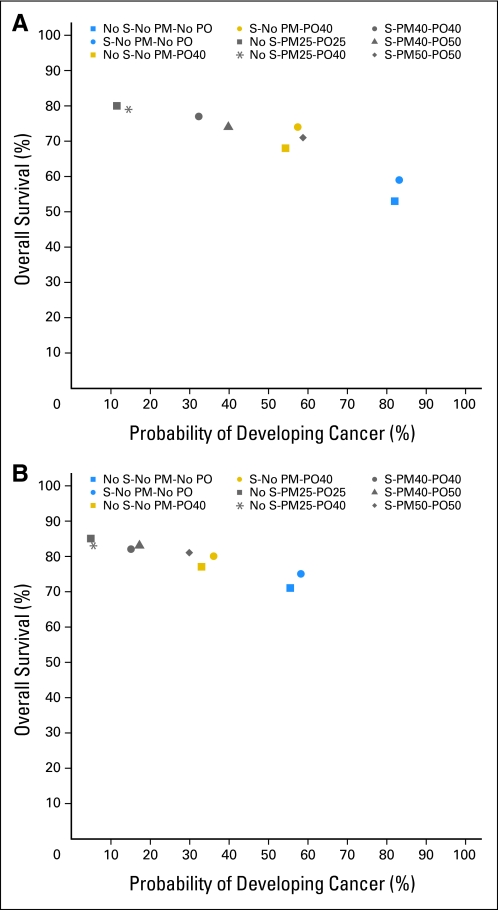
Results: We compared strategies on cancer incidence and survival to age 70 years; for example, PO plus PM at age 25 years optimizes both outcomes (incidence, 4% to 11%; survival, 80% to 83%), whereas PO at age 40 years plus MRI screening offers less effective prevention, yet similar survival (incidence, 36% to 57%; survival, 74% to 80%). To characterize patients' treatment and survivorship experiences, we reported the tumor features and treatments associated with risk-reducing interventions; for example, in most BRCA2 mutation carriers (81%), MRI screening diagnoses stage I, hormone receptor-positive breast cancers, which may not require chemotherapy.
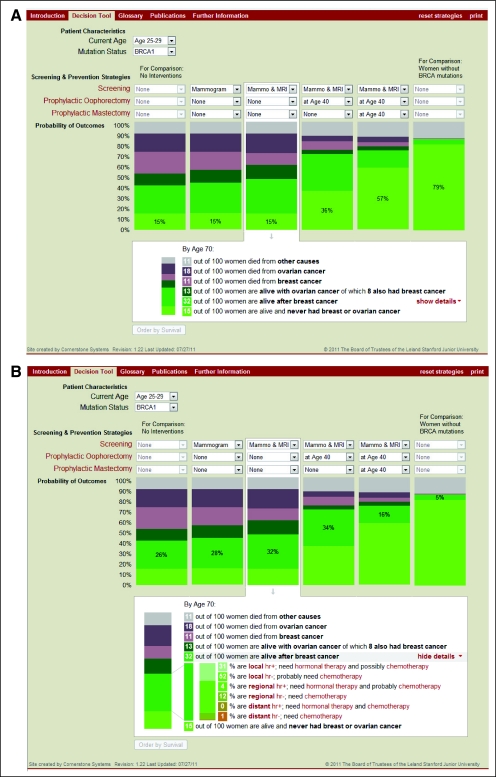
Conclusion: Cancer risk-reducing options for BRCA1/2 mutation carriers vary in their impact on cancer incidence, recommended treatments, quality of life, and survival. To guide decisions informed by multiple health outcomes, we provide an online tool for joint use by patients with their physicians (http://brcatool.stanford.edu).
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

Comment in
-
Are we ready for online tools in decision making for BRCA1/2 mutation carriers?J Clin Oncol. 2012 Feb 10;30(5):471-3. doi: 10.1200/JCO.2011.40.1562. Epub 2012 Jan 9. J Clin Oncol. 2012. PMID: 22231044 No abstract available.
References
-
- Domchek SM, Friebel TM, Neuhausen SL, et al. Mortality after bilateral salpingo-oophorectomy in BRCA1 and BRCA2 mutation carriers: A prospective cohort study. Lancet Oncol. 2006;7:223–229. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
